All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q251
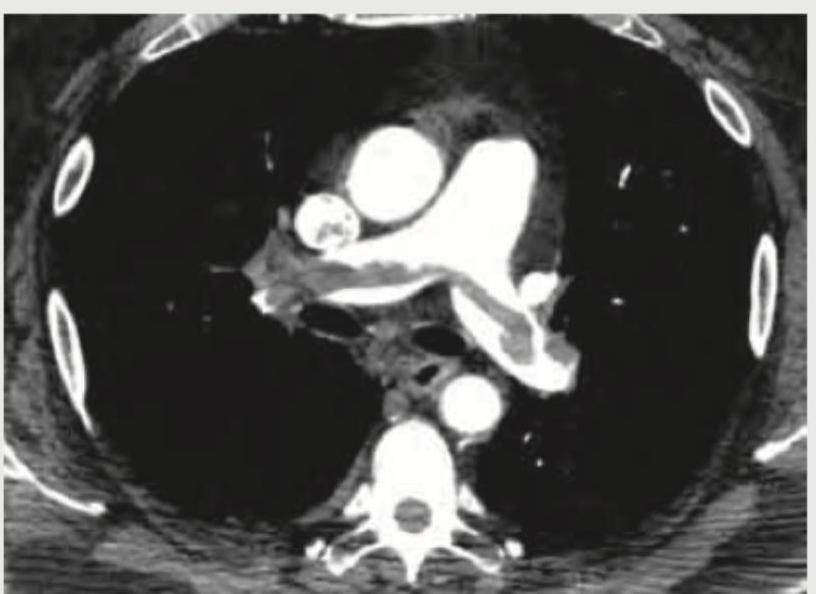
A 35-year-old male with history of 4 weeks of immobilization for fracture of femur develops sudden onset breathlessness and blood in sputum. CT angiography shows? (Recent NEET Pattem 2018-19)