All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q191
All of the following characteristic patterns seen in Brown-Sequard syndrome; except:-
Q192
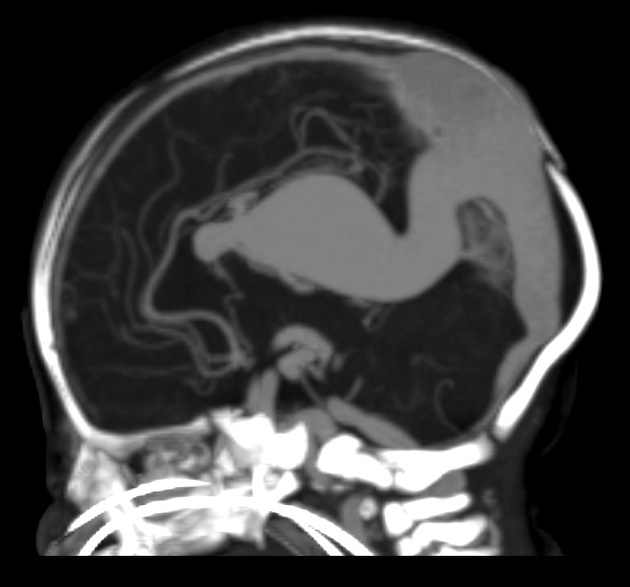
A newborn male baby presents with congestive heart failure. On examination, there are enlarged fontanelles, a loud cranial bruit, and the following radiological finding. What is the most likely diagnosis?