All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q171
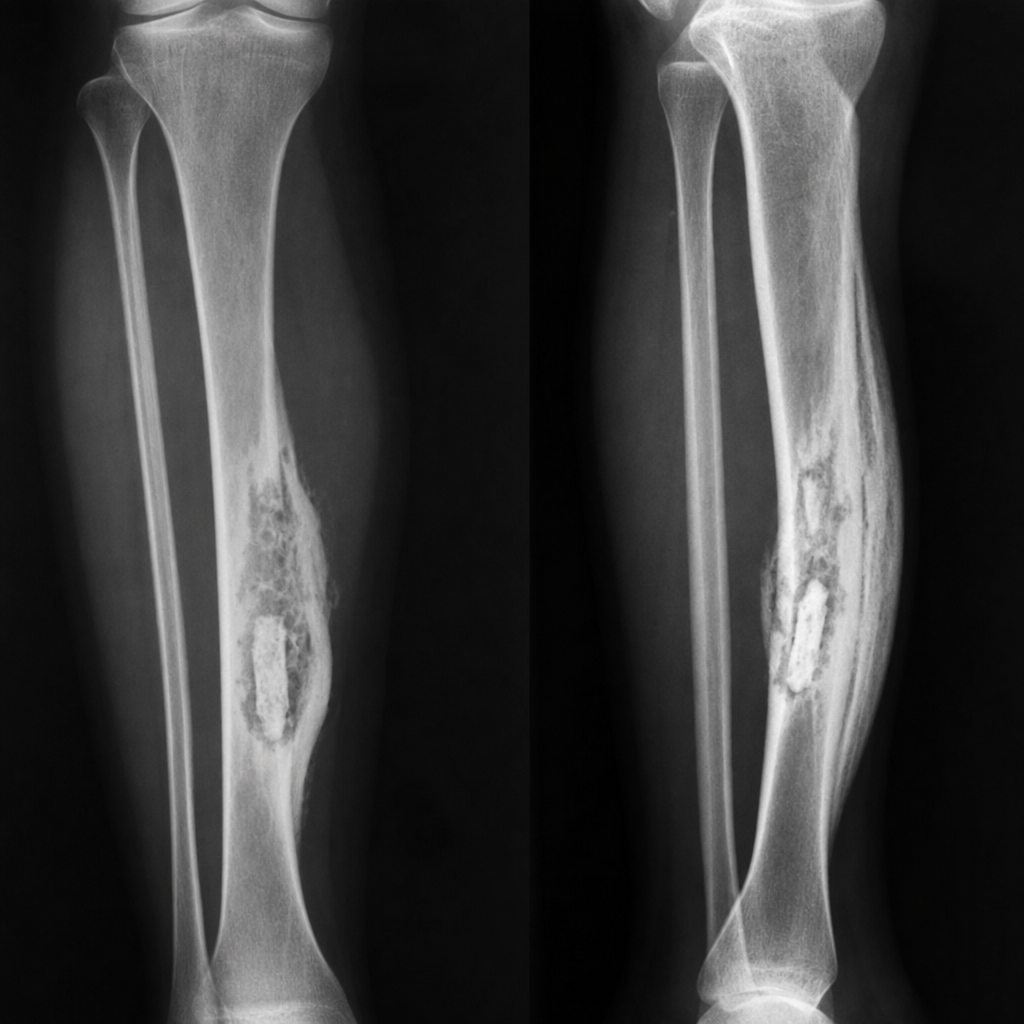
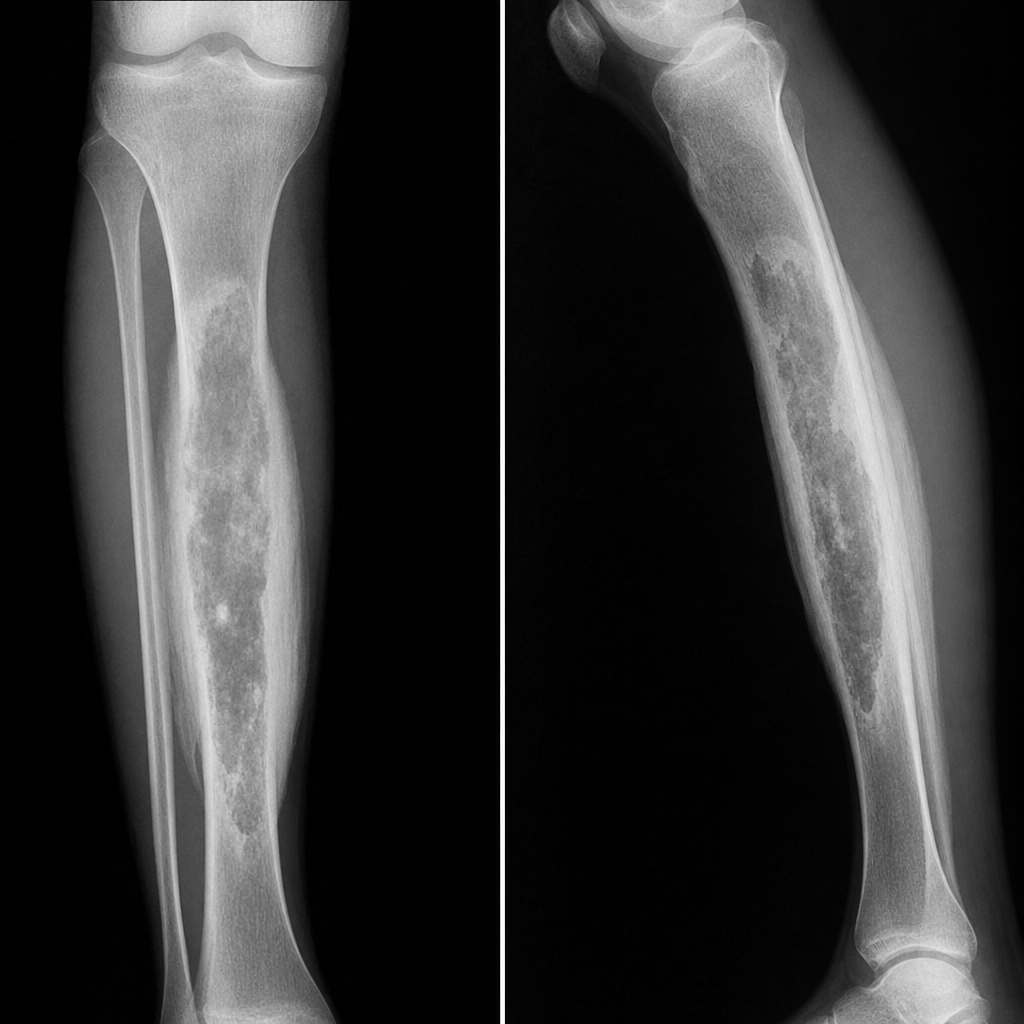
A patient has a history of RTA 2 years ago. He developed pain and swelling at the same site. What will be the diagnosis based on the provided X-ray features?
Q172
A patient had osteomyelitis in their left tibia 2 years ago. They now present with pain and swelling at the same site. X-ray shows bone destruction, sequestrum, and involucrum. What is the most likely diagnosis?