All SubjectsAnatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q11
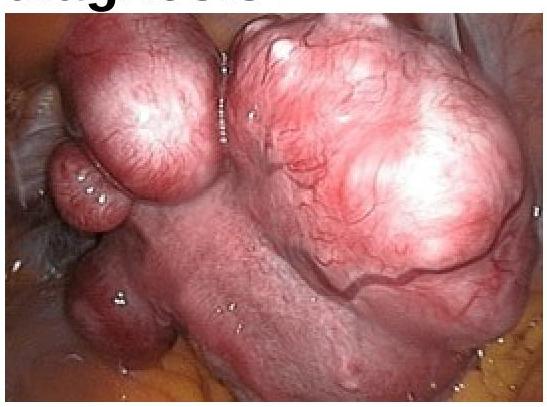
In a woman complaining of AUB following image was seen in endoscopic examination of uterus. What will be the diagnosis?
Q12
Which drug regimen is given to a pregnant woman with HIV infection?
Q13
Which of the following statements about the placenta is correct?
Q14
What is the most common symptom treated with hormone therapy (HT) in menopausal women?
Q15
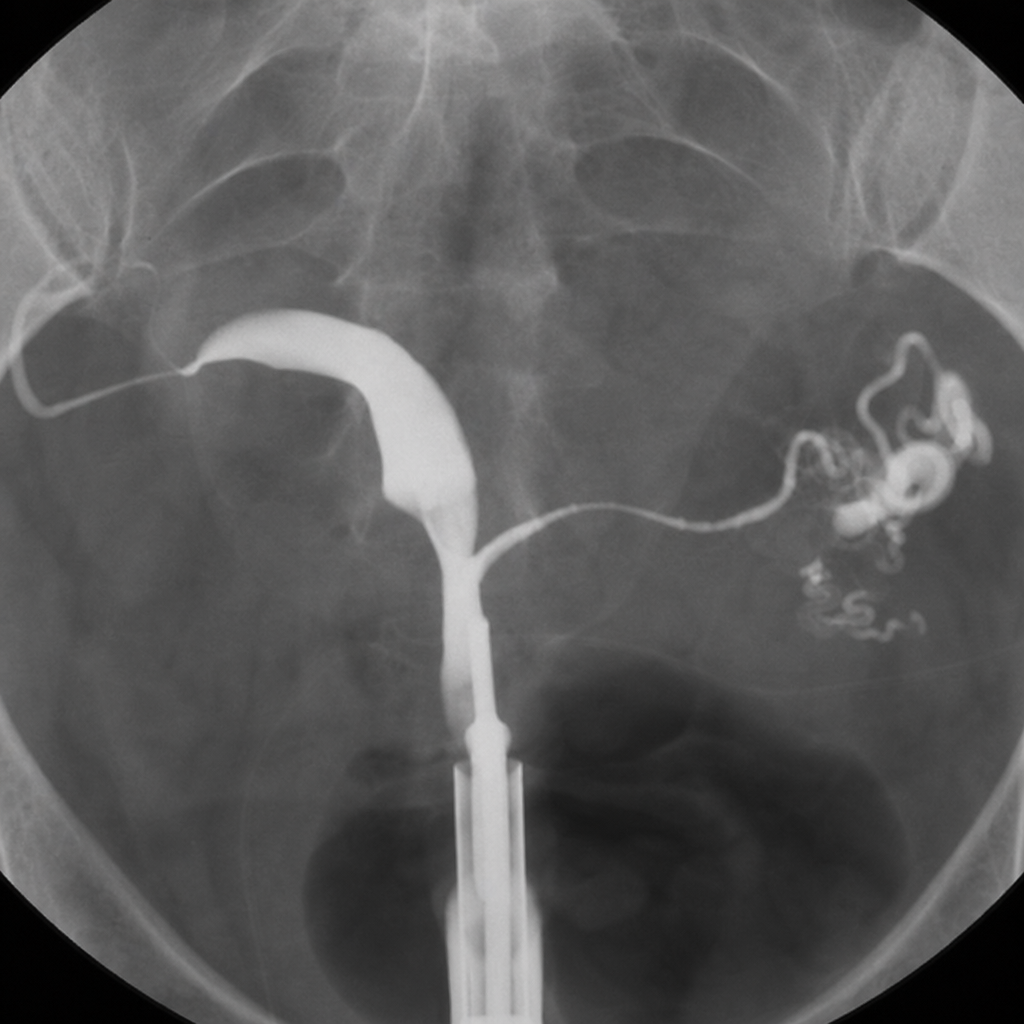
Identify the X-ray HSG image shown below:
Q16
Based on the provided image, which of the following is the correct diagnosis?

Q17
Which of the following is the most common cause of perforation of uterus in non-pregnant state?
Q18
A 16-year-old girl comes to you with primary amenorrhea; on evaluation there is absent breast development, she has a normal stature, her FSH and LH levels are found to be high and she has a karyotype of 46XX. What is the probable diagnosis?
Q19
Shoulder dystocia is managed by all of the following except:-
Q20
In Peripartum cardiomyopathy, cardiac failure occurs at:-