All SubjectsAnatomy (24)Anesthesiology (4)Biochemistry (1)Biochemistry (26)Community Medicine (12)Dental (1)Dermatology (8)ENT (1)Forensic Medicine (2)General Medicine (7)Internal Medicine (41)Microbiology (22)Obstetrics and Gynecology (23)Ophthalmology (2)Orthopaedics (1)Pathology (3)Pathology (31)Pediatrics (24)Pharmacology (27)Physiology (13)Psychiatry (3)Psychiatry (10)Radiology (30)Surgery (5)Surgery (32)
Q31
Factor V mutation most commonly initially presents as:-
Q32
Which of the following conditions is most commonly associated with cryoglobulinemia?
Q33
Which of the following is seen in Rheumatoid Arthritis?
Q34
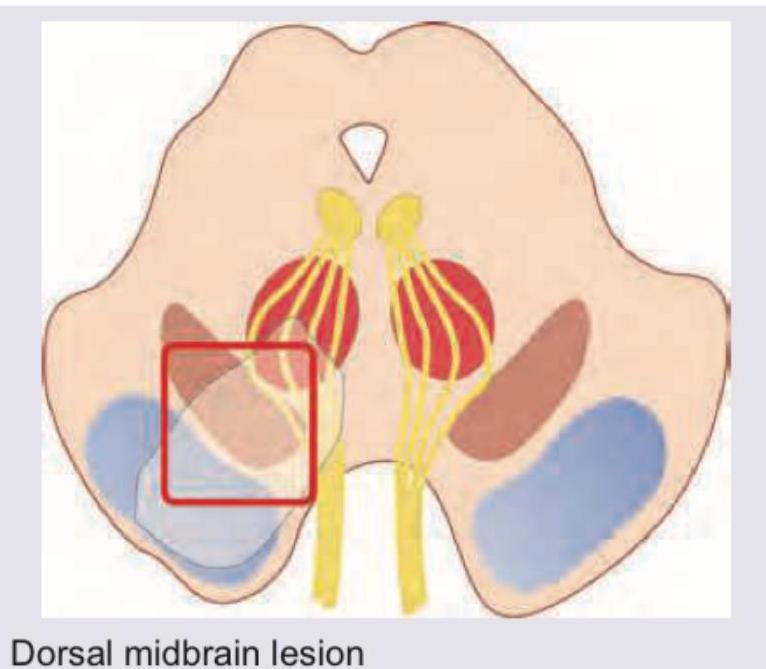
All are true about the mid brain stroke syndrome shown except:
Q35
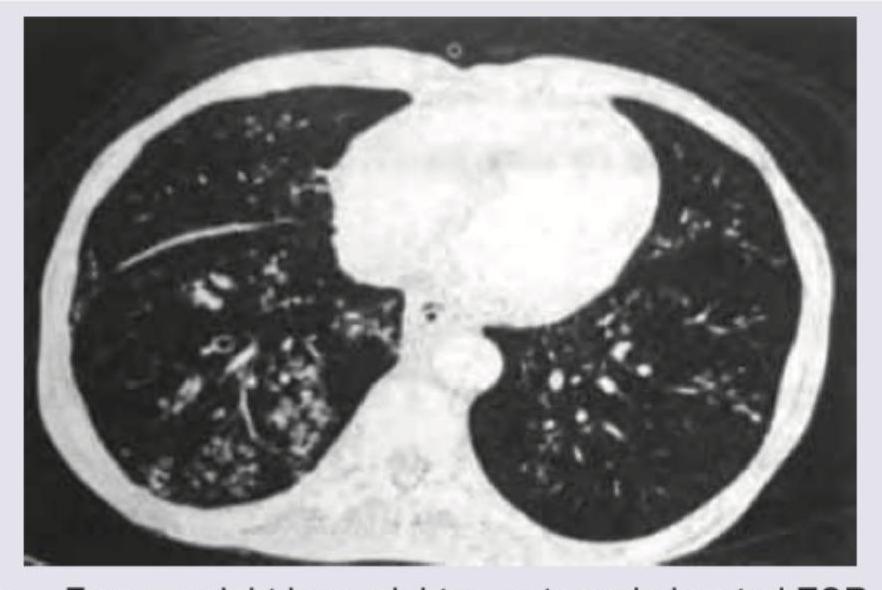
A patient in ICU was given blood transfusion. 3 hours later SpO2 is reduced to 75% with respiratory difficulty. CVP is 15 cm water and PCWP is 25 mm Hg . CXR is shown below. What is the diagnosis?

Q36
A patient undergone a Solid organ transplant is having the following lesions which are present on oral mucosa and sites shown below. Which of the following is incriminated in causing the same?

Q37
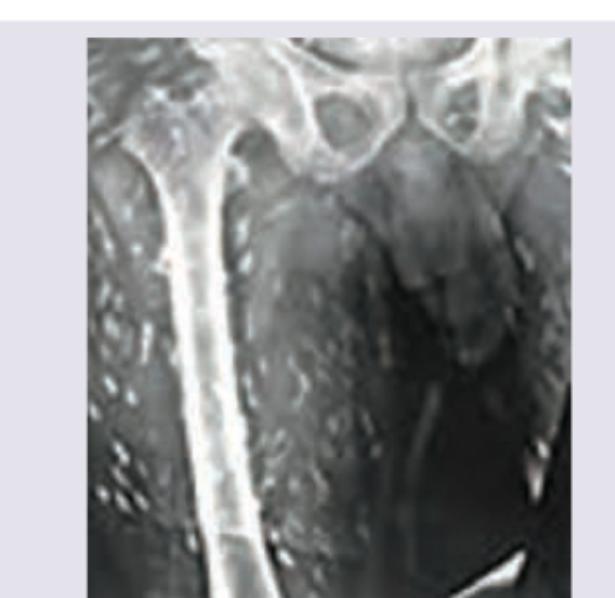
The finding shown below is used for diagnosis of CNS parasitic lesion. Which of the following best describes the condition?
Q38
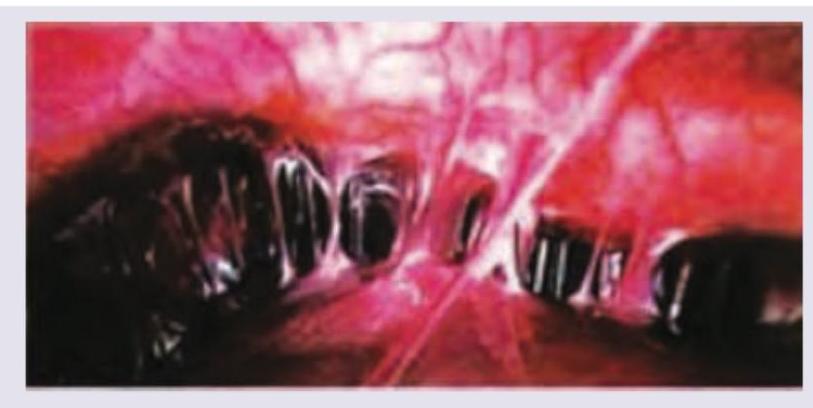
Which one of the following is implicated in the etiology of these adhesions around the liver?
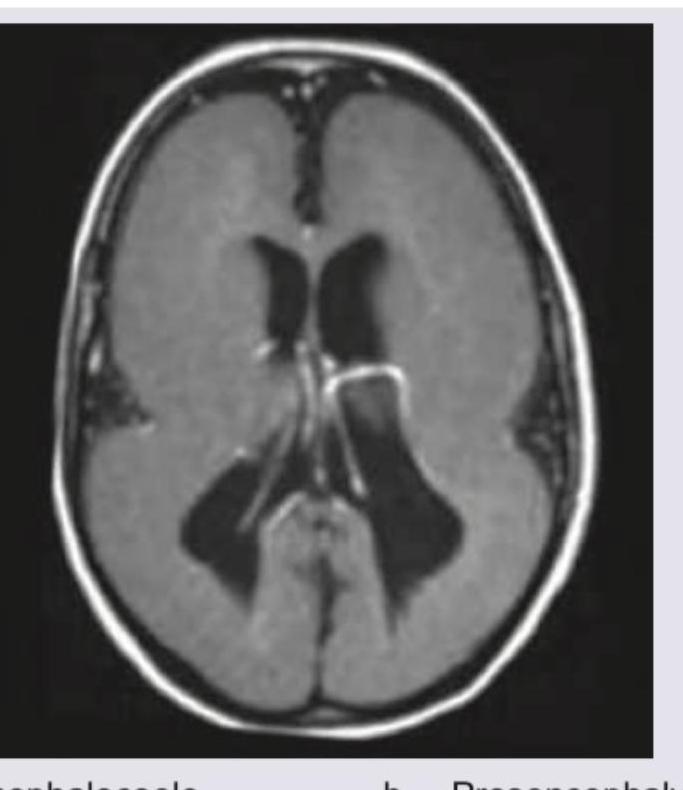
Q39
Identify the following abnormality?
Q40
Which of the following will best describe this patient?