Stunning of myocardium without any acute coronary syndrome is:-
Mean transformation time for HIV to AIDS is:-
All of the following characteristic patterns seen in Brown-Sequard syndrome; except:-
Falsely elevated ankle brachial index is used for evaluation of?
A newborn male baby presents with congestive heart failure. On examination, there are enlarged fontanelles, a loud cranial bruit, and the following radiological finding. What is the most likely diagnosis?
VMA is elevated in which of the following condition?
All of the following are true about ulcerative colitis except:
Which of the following hematological problems may be precipitated by parvovirus?
True statement regarding upper GI bleeds:
Which of the following is not true regarding Von Willebrand disease?
NEET-PG 2018 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 21: Stunning of myocardium without any acute coronary syndrome is:-
- A. Restrictive cardiomyopathy
- B. Subendocardial infarction
- C. Transmural infarction
- D. Takotsubo cardiomyopathy (Correct Answer)
Explanation: ***Takotsubo cardiomyopathy*** - This condition involves **transient systolic dysfunction** of the left ventricle, often triggered by severe emotional or physical stress, mimicking a heart attack but without **coronary artery obstruction**. - The apical and mid-ventricular segments of the left ventricle become akinetic or hypocinetic, causing the heart to take on a shape resembling an octopus trap (**takotsubo**). *Restrictive cardiomyopathy* - This is a condition where the walls of the ventricles become **stiff** and **lose their flexibility**, preventing the heart from filling properly. - It is typically caused by conditions like **amyloidosis** or **sarcoidosis**, leading to impaired diastolic function, not transient stunning. *Subendocardial infarction* - This refers to a **heart attack** that affects only the **inner layer** of the heart muscle (**subendocardium**) due to reduced blood flow [2]. - It is a form of **acute coronary syndrome** where there is irreversible myocardial necrosis, unlike the temporary dysfunction in stunning [1]. *Transmural infarction* - This is a **severe form of heart attack** where the entire thickness of the heart muscle wall is affected, usually due to a **complete blockage of a coronary artery** [2]. - This also represents **acute coronary syndrome** with widespread myocardial necrosis, which is fundamentally different from a reversible stunning of the myocardium [1].
Question 22: Mean transformation time for HIV to AIDS is:-
- A. 12 years
- B. 9 years
- C. 5 years
- D. 10 years (Correct Answer)
Explanation: ***10 years*** - The mean transformation time from initial **HIV infection** to the development of **AIDS** in untreated individuals is approximately 10 years [1]. - This time frame represents the average duration of the **clinical latency period**, during which the viral load increases and CD4+ T-cell count gradually declines [1]. *12 years* - While some individuals may progress to AIDS later than 10 years, 12 years is not recognized as the **mean transformation time**. - This longer period might be seen in individuals with slower disease progression or those initiating **antiretroviral therapy (ART)** at later stages. *9 years* - This duration is slightly shorter than the generally accepted mean, though some individuals may progress more rapidly. - Factors like **higher viral load** at infection, coinfections, or certain genetic predispositions can accelerate progression. *5 years* - A transformation time of 5 years is considered a **rapid progression** to AIDS. - This rapid progression is typically seen in a minority of HIV-infected individuals, often associated with factors such as high baseline viral load, genetic susceptibility, or co-infection with other pathogens.
Question 23: All of the following characteristic patterns seen in Brown-Sequard syndrome; except:-
- A. Contralateral loss of pain and temperature
- B. Ipsilateral weakness
- C. Ipsilateral loss of position and vibration
- D. Ipsilateral loss of pain and temperature (Correct Answer)
Explanation: ***Ipsilateral loss of pain and temperature*** - Brown-Sequard syndrome results from **hemitransverse spinal cord lesion**, leading to distinct sensory and motor deficits on only one side of the body [1]. - Pain and temperature pathways (spinothalamic tracts) **decussate (cross over)** in the spinal cord upon entry, so a lesion on one side causes **contralateral** loss of these sensations [2]. *Contralateral loss of pain and temperature* - This is a **characteristic finding** in Brown-Sequard syndrome, as the spinothalamic tracts (carrying pain and temperature) cross over at the level of the spinal cord [2]. - A lesion on one side of the spinal cord therefore results in the loss of these sensations on the **opposite side of the body below the level of the lesion** [1]. *Ipsilateral weakness* - This is a **characteristic finding** in Brown-Sequard syndrome due to the involvement of the **corticospinal tracts** (responsible for motor function) [1]. - These tracts primarily descend **uncrossed** in the spinal cord, so a lesion on one side causes weakness on the **same side of the body below the level of the lesion**. *Ipsilateral loss of position and vibration* - This is a **characteristic finding** in Brown-Sequard syndrome because the **dorsal columns** (medial lemniscal pathway), responsible for fine touch, proprioception, and vibration, ascend **ipsilaterally (uncrossed)** in the spinal cord [2]. - A lesion on one side of the spinal cord therefore results in the loss of these sensations on the **same side of the body below the level of the lesion** [1].
Question 24: Falsely elevated ankle brachial index is used for evaluation of?
- A. Deep vein thrombosis
- B. Acute limb ischemia
- C. Calcified vessels (Correct Answer)
- D. Chronic venous insufficiency
Explanation: A falsely elevated **ankle-brachial index (ABI)**, often >1.3, indicates that the **ankle arteries are non-compressible** due to calcification [1]. This calcification is common in conditions like **diabetes** and **end-stage renal disease**, where the vessels become stiff and resist compression, leading to inaccurate pressure readings [1].
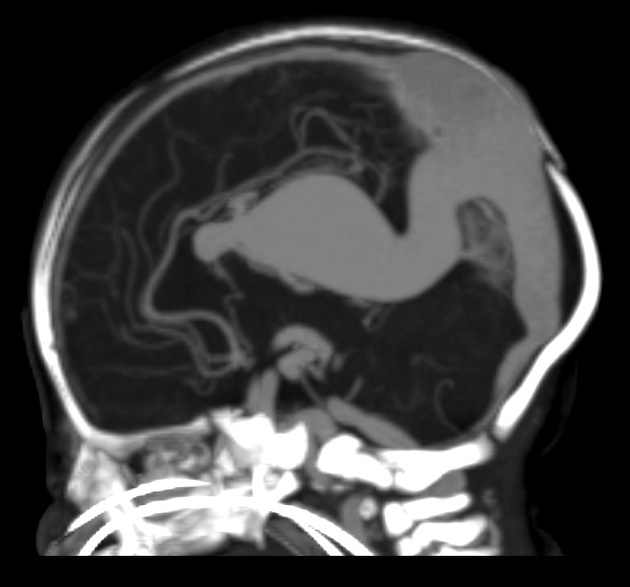
Question 25: A newborn male baby presents with congestive heart failure. On examination, there are enlarged fontanelles, a loud cranial bruit, and the following radiological finding. What is the most likely diagnosis?
- A. Pneumocephalus
- B. Crouzon syndrome
- C. Dandy walker syndrome
- D. Vein of Galen malformation (Correct Answer)
Explanation: ***Vein of Galen malformation*** - The imaging displays a massively dilated **vein of Galen**, indicating a **Vein of Galen malformation (VOGM)**. - VOGM creates a large **arteriovenous shunt**, leading to high-output **congestive heart failure** and often presenting with prominent **cranial bruits** and **macrocephaly** (enlarged fontanelles). *Pneumocephalus* - This condition involves the presence of **air within the intracranial cavity**, commonly due to trauma, surgery, or infection. - It would not explain the **congestive heart failure** or the vascular malformation seen on the imaging. *Crouzon syndrome* - This is a form of **craniosynostosis** characterized by abnormalities in skull and facial bone development, including **midfacial hypoplasia** and **proptosis**. - While it can involve enlarged fontanelles due to hydrocephalus, it does not typically cause **congestive heart failure** or a **cranial bruit** from a vascular malformation. *Dandy-Walker syndrome* - This congenital brain malformation involves agenesis or hypoplasia of the **cerebellar vermis** and cystic dilation of the **fourth ventricle**, often leading to hydrocephalus. - While it can cause enlarged fontanelles, it does not typically lead to **congestive heart failure** or a **cranial bruit**, nor does it present with the characteristic vascular lesion seen in the image.
Question 26: VMA is elevated in which of the following condition?
- A. Tuberous sclerosis
- B. Addison disease
- C. Pheochromocytoma (Correct Answer)
- D. Conn Syndrome
Explanation: Pheochromocytoma - Pheochromocytoma is a tumor of the adrenal medulla that secretes excessive amounts of catecholamines (epinephrine and norepinephrine). - Vanillylmandelic acid (VMA) is a breakdown product of these catecholamines [1], so its levels are elevated in the urine of patients with pheochromocytoma. Tuberous sclerosis - Tuberous sclerosis is a genetic disorder characterized by the growth of numerous non-cancerous tumors in various organs. - While it can be associated with renal angiomyolipomas or brain lesions, it does not directly cause elevated VMA levels. Addison disease - Addison disease is characterized by adrenal insufficiency [2], meaning the adrenal glands produce insufficient amounts of hormones like cortisol and aldosterone. - This condition is not associated with the overproduction of catecholamines or elevated VMA. Conn Syndrome - Conn syndrome (primary hyperaldosteronism) is due to an overproduction of aldosterone by the adrenal glands, often caused by an adrenal adenoma [3]. - Aldosterone is a mineralocorticoid, and its overproduction does not lead to increased catecholamine metabolism or elevated VMA levels.
Question 27: All of the following are true about ulcerative colitis except:
- A. Surgery is required in a subset of severe cases.
- B. Extra-intestinal problems of UC are managed medically
- C. The highest risk of UC requiring surgery in 1st year
- D. Steroid dependent cases need surgery (Correct Answer)
Explanation: ***Steroid dependent cases need surgery*** - While **steroid dependency** in ulcerative colitis (UC) indicates a need for alternative or escalate medications, it does not automatically necessitate surgery [1]. - Many steroid-dependent patients can be managed effectively with **immunomodulators** or **biologic therapies**, avoiding surgery. *Surgery is required in a subset of severe cases.* - **Severe ulcerative colitis** that is refractory to medical therapy, or complicated by toxic megacolon, perforation, or severe bleeding, often requires surgical intervention [1]. - This statement is true, as surgery can be curative for UC by removing the affected colon [1]. *Extra-intestinal problems of UC are managed medically* - **Extra-intestinal manifestations** of ulcerative colitis, such as arthritis, skin lesions (erythema nodosum), and eye inflammation (uveitis), are typically managed with medications specific to those conditions, often in conjunction with UC treatment [1], [2]. - This statement is true, as these manifestations rarely require surgical intervention themselves. *The highest risk of UC requiring surgery in 1st year* - The risk of surgery in ulcerative colitis is indeed highest in the **first year after diagnosis**, particularly for patients presenting with severe disease. - This initial period often determines the disease course and responsiveness to medical treatment.
Question 28: Which of the following hematological problems may be precipitated by parvovirus?
- A. Aplastic crisis (Correct Answer)
- B. Hemolytic crisis
- C. Thrombocytopenia
- D. Pancytopenia
Explanation: ***Aplastic crisis*** - Parvovirus B19 preferentially infects and destroys **erythroid progenitor cells** in the bone marrow, leading to a temporary halt in red blood cell production [1]. - This can precipitate an **aplastic crisis**, especially in individuals with underlying chronic hemolytic anemias (e.g., **sickle cell disease** or **hereditary spherocytosis**), where red blood cell lifespan is already shortened [2]. *Hemolytic crisis* - A hemolytic crisis involves an **accelerated destruction of red blood cells**, leading to a sudden drop in hemoglobin. - While parvovirus can indirectly worsen anemia, it primarily affects red cell production rather than directly increasing their destruction, acting more as a trigger for a production problem than a hemolytic one [1]. *Thrombocytopenia* - **Thrombocytopenia** is characterized by a low platelet count, which can lead to bleeding disorders. - While viral infections can sometimes cause mild myelosuppression affecting platelets, parvovirus B19 is not typically associated with severe or primary thrombocytopenia. *Pancytopenia* - **Pancytopenia** is a reduction in all three blood cell lines (red blood cells, white blood cells, and platelets). - While parvovirus can cause a transient aplastic crisis (affecting red cells), it rarely causes a severe, sustained suppression of all cell lines to be classified as true pancytopenia, though some transient leukopenia may occur [1].
Question 29: True statement regarding upper GI bleeds:
- A. Upper GI bleeding is defined as bleeding originating proximal to the ampulla of Vater, not the ligament of Treitz
- B. Endoscopic banding is the first-line treatment for all types of upper GI bleeding
- C. The most common cause of upper GI bleeds is peptic ulcer disease, not variceal bleeding. (Correct Answer)
- D. Rockall score is primarily used for immediate treatment decisions rather than risk stratification
Explanation: ***The most common cause of upper GI bleeds is peptic ulcer disease, not variceal bleeding.*** [1] * **Peptic ulcer disease (PUD)**, particularly **duodenal and gastric ulcers**, accounts for the majority of upper GI bleeding cases. * While **variceal bleeding** is severe and life-threatening, it is a less frequent cause overall compared to PUD. *Endoscopic banding is the first-line treatment for all types of upper GI bleeding* * **Endoscopic banding** is primarily indicated and highly effective for **esophageal variceal bleeding**, not for all types of upper GI bleeds. * For non-variceal bleeding, such as **peptic ulcers**, treatments like **epinephrine injection**, **heater probe**, or **clips** are more commonly utilized [1]. *Upper GI bleeding is defined as bleeding originating proximal to the ampulla of Vater, not the ligament of Treitz* * **Upper GI bleeding** is classically defined as bleeding occurring **proximal to the ligament of Treitz**, which marks the anatomical division between the duodenum and the jejunum. * The **ampulla of Vater** is located in the second part of the duodenum, and bleeding upstream of this point is still considered upper GI bleed. *Rockall score is primarily used for immediate treatment decisions rather than risk stratification* * The **Rockall score** is a validated tool specifically designed for **risk stratification** in upper GI bleeding, predicting rebleeding and mortality [1]. * While it informs overall management, immediate treatment decisions are often guided by the patient's **hemodynamic stability** and endoscopic findings, rather than solely by the score.
Question 30: Which of the following is not true regarding Von Willebrand disease?
- A. Normal platelet count
- B. Quantitative defects are seen in subtypes 1 and 3 von Willebrand disease
- C. Produced by endothelial cells
- D. Hemarthrosis is the usual presentation (Correct Answer)
Explanation: **Hemarthrosis is the usual presentation** - **Hemarthrosis** (bleeding into joints) is characteristic of severe factor deficiencies, such as **hemophilia A or B**, but is uncommon in von Willebrand disease (vWD) [2]. - vWD typically presents with **mucocutaneous bleeding** (e.g., easy bruising, nosebleeds, heavy menstrual bleeding) due to impaired platelet adhesion [2]. *Normal platelet count* - Patients with von Willebrand disease usually have a **normal platelet count**, as the issue is with the function or quantity of **von Willebrand factor (vWF)**, not the number of platelets [3]. - vWF primarily mediates platelet adhesion and protects **factor VIII** from degradation, so platelet production itself is unaffected [1]. *Quantitative defects are seen in subtypes 1 and 3 von Willebrand disease* - **Type 1 vWD** involves a partial **quantitative deficiency** of vWF, meaning reduced levels of otherwise normal vWF. - **Type 3 vWD** is characterized by a severe or near-complete **absence of vWF**, representing the most severe quantitative defect. *Produced by endothelial cells* - **Von Willebrand factor (vWF)** is primarily synthesized and stored in **endothelial cells** (in Weibel-Palade bodies) and also in **megakaryocytes**. - Its production by endothelial cells allows for its release into the bloodstream and subendothelial matrix to facilitate **hemostasis**.