All SubjectsAnatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q11
Patient presenting with cutaneous vasculitis, glomerulonephritis, peripheral neuropathy, Which investigation is to be performed next that will help you diagnose the condition?
Q12
Which drug is used as an adjunct to epinephrine in refractory ventricular fibrillation/ventricular tachycardia during cardiac arrest?
Q13
Which is not included in AIDS related complex?
Q14
Which of the following is the MOST characteristic feature of ataxia telangiectasia?
Q15
Which condition is associated with the ECG pattern known as pseudo P pulmonale?
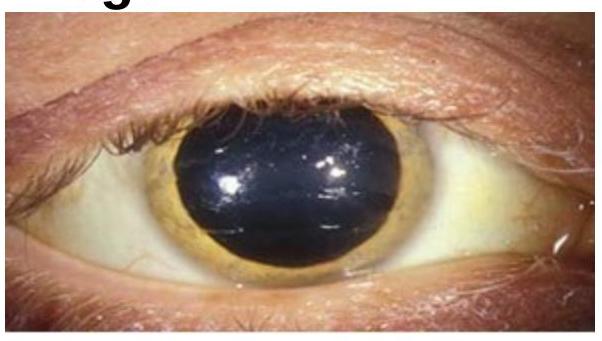
Q16
Choose the best method of diagnosis for the clinical sign represented in the image.
Q17
What is a potential cause of cardiogenic shock other than myocardial infarction (MI)?
Q18
What is the earliest feature of third cranial nerve involvement in a patient with diabetes mellitus?
Q19
Stunning of myocardium without any acute coronary syndrome is:-
Q20
Mean transformation time for HIV to AIDS is:-