NEET-PG 2018 — Dermatology
8 Previous Year Questions with Answers & Explanations
Which of the following are risk factors for cutaneous lymphoma?
Cutis marmorata occurs due to exposure to –
Which of the following statements about keloids is MOST true?
Identify the skin lesion shown in the image.

Comment on the image shown:

A 24-year-old male presents with a lesion at the site shown in the image for 4 years. He says it has increased in thickness over the years. Diagnosis is:

Which of the following layers is absent in psoriasis?
Which of the following layers contains Odland bodies?
NEET-PG 2018 - Dermatology NEET-PG Practice Questions and MCQs
Question 1: Which of the following are risk factors for cutaneous lymphoma?
- A. Weakened immune system
- B. Age
- C. Gender
- D. All of the options (Correct Answer)
Explanation: ***All of the options*** - **All listed factors**, including age, gender, and a weakened immune system, are recognized risk factors for the development of cutaneous lymphoma. - The risk of cutaneous lymphoma generally **increases with age**, shows a slightly higher incidence in **males**, and is significantly elevated in individuals with **compromised immune systems**. *Age* - While age is a risk factor, it is only one component among several that contribute to the overall risk of developing cutaneous lymphoma. - The incidence of most lymphomas, including cutaneous forms, typically **increases with advancing age**, but other factors also play a critical role. *Gender* - Like age, gender is a recognized risk factor, with a slightly **higher incidence in males** compared to females. - However, gender alone does not fully explain the risk, as environmental and other host-related factors also contribute. *Weakened immune system* - A weakened immune system is a significant risk factor, as it impairs the body's ability to control abnormal cell growth, including cancerous lymphocytes. - However, it is not the sole risk factor; individuals with healthy immune systems can also develop cutaneous lymphoma due to other contributing factors.
Question 2: Cutis marmorata occurs due to exposure to –
- A. Cold temperature (Correct Answer)
- B. Dust
- C. Hot temperature
- D. Humidity
Explanation: ***Cold temperature*** - **Cutis marmorata** is a physiological response to **cold temperatures**, characterized by a mottled, reticulated vascular pattern on the skin. - This occurs due to **vasoconstriction** of the small arteries and arterioles, alongside **vasodilation** of the venules, creating the characteristic marbled appearance. *Dust* - Exposure to **dust** typically causes **irritation**, allergic reactions, or respiratory issues, such as **dermatitis**, **contact urticaria**, or **asthma**. - It does not directly lead to the characteristic vascular changes seen in cutis marmorata. *Hot temperature* - **Hot temperatures** generally cause **vasodilation** in the skin to facilitate **heat dissipation**, leading to redness and warmth. - This is the opposite physiological response to cutis marmorata, which involves vasoconstriction. *Humidity* - **Humidity** primarily affects **skin hydration** and the rate of perspiration, potentially exacerbating certain skin conditions like **eczema** or **fungal infections**. - High or low humidity does not directly induce the vascular changes that result in cutis marmorata.
Question 3: Which of the following statements about keloids is MOST true?
- A. Keloids may extend beyond the original wound. (Correct Answer)
- B. Extended excision is often not the treatment of choice.
- C. It contains growth factors.
- D. None of the options.
Explanation: ***Keloids may extend beyond the original wound.*** - Keloids are characterized by their **overgrowth** beyond the boundaries of the original injury. - This distinguishes them from **hypertrophic scars**, which remain confined to the wound edges. *Extended excision is often not the treatment of choice.* - **Excision alone** is usually insufficient for keloids and can even be counterproductive, as the recurring wound often leads to a larger keloid. - While excision can be part of a treatment plan, it is typically combined with supplementary therapies like **steroid injections** or **radiation therapy** to prevent recurrence. *It contains growth factors.* - While keloids involve abnormal fibroblast activity and deposition of **extracellular matrix**, the statement that it "contains growth factors" is too vague and not a defining characteristic that differentiates it from a range of other tissues or conditions. - Many tissues and healing processes involve growth factors, so this statement alone does not provide a specific or most true characteristic of keloids. *None of the options.* - This option is incorrect because the statement that **keloids may extend beyond the original wound** is a hallmark characteristic of keloids and is definitively true.
Question 4: Identify the skin lesion shown in the image.
- A. Becker nevus (Correct Answer)
- B. Hypopigmented macule
- C. Spitz nevus
- D. Epidermal nevus
Explanation: ***Becker nevus*** - This image clearly shows a large, **hyperpigmented patch with overlying coarse terminal hairs**, characteristic of a Becker nevus. - Becker nevi typically develop in adolescence and are often found on the shoulder or upper trunk, as seen here. *Hypopigmented macule* - A **hypopigmented macule** would appear as an area of skin with **reduced pigmentation** (lighter than the surrounding skin), which is contrary to the darker lesion shown. - There would also be no indication of **increased hair growth** within a typical hypopigmented macule. *Spitz nevus* - A Spitz nevus is a benign melanocytic nevus often appearing as a **dome-shaped, pink or red papule or nodule**, commonly on the face or limbs. - It does not present as a large, hairy, **hyperpigmented patch** as depicted in the image. *Epidermal nevus* - An epidermal nevus is a **congenital lesion** formed by an overgrowth of epidermal cells, but its appearance is typically a **verrucous (wart-like) plaque** or linearly arranged papules. - While it can be hyperpigmented, it generally **lacks the prominent hypertrichosis** (excessive hair growth) seen in the image.
Question 5: Comment on the image shown:
- A. Corn
- B. Callosity
- C. Warts
- D. Cutaneous horn
- E. Arsenical keratosis (Correct Answer)
Explanation: ***Arsenical keratosis*** - The image shows characteristic **raindrop pigmentation** (alternating hypo/hyperpigmented macules) and **palmar/plantar keratoses** pathognomonic of chronic **arsenic toxicity**. - Associated with **Blackfoot disease** (peripheral vascular disease) and increased risk of **skin malignancies**, distinguishing it from benign hyperkeratotic conditions. *Corn* - A corn presents as a **single, localized lesion** with a **painful central core**, unlike the multiple diffuse keratotic lesions with pigmentary changes seen here. - Corns are **friction-induced** and lack the characteristic **raindrop pigmentation** associated with arsenic exposure. *Callosity* - Callosity results from **repeated friction and pressure** causing broad, flat hyperkeratotic thickening without pigmentary changes. - It lacks the **alternating hypo/hyperpigmented macules** and **corn-like keratoses** characteristic of arsenical toxicity. *Warts* - **Viral warts** caused by **HPV** show **black puncta** (thrombosed capillaries) and **papillomatous surface** upon examination. - They present as **elevated, rough lesions** without the **raindrop pigmentation** and flat keratotic appearance of arsenical keratosis. *Cutaneous horn* - A **cutaneous horn** appears as a **solitary, conical projection** of keratin resembling an animal horn, typically on sun-exposed areas. - It presents as a **single horn-like protrusion** rather than the **multiple flat keratoses** with pigmentary changes shown in arsenical keratosis.
Question 6: A 24-year-old male presents with a lesion at the site shown in the image for 4 years. He says it has increased in thickness over the years. Diagnosis is:
- A. Spitz nevus
- B. Hyper-melanosis of Ito
- C. Becker's nevus (Correct Answer)
- D. Congenital melanocytic nevus
Explanation: ***Becker's nevus*** - This lesion typically presents as a **unilateral, hyperpigmented patch** that often appears during childhood or adolescence, increasing in size and thickness with associated **hypertrichosis** (increased hair growth). The image shows a large, irregularly shaped, hyperpigmented area on the torso of a young male, consistent with this description. - The history of increasing thickness over four years further supports **Becker's nevus**, as it is known to progress in thickness and texture, often becoming more indurated and sometimes verrucous. *Spitz nevus* - Spitz nevus is a benign melanocytic nevus typically presenting as a **pink or red, dome-shaped papule or nodule**, commonly on the face or limbs. - It rapidly grows but does not typically present as a large, hyperpigmented patch with associated hypertrichosis like the lesion shown. *Hyper-melanosis of Ito* - Hypermelanosis of Ito (also known as incontinentia pigmenti achromians) is characterized by **streaky or whorled hypopigmented (lighter) skin lesions**, often present at birth or in early infancy. - The image clearly shows a **hyperpigmented (darker) lesion**, which directly contradicts the characteristic hypopigmentation of hypermelanosis of Ito. *Congenital melanocytic nevus* - Congenital melanocytic nevi are typically present **at birth** or become apparent shortly thereafter. While they can be large and hyperpigmented, they usually do not have the prominent feature of increasing thickness and hypertrichosis developing many years later in adolescence or early adulthood in the same way as Becker's nevus. - The description of a lesion appearing during adolescence and increasing in thickness and hairiness for four years makes Becker's nevus a more specific diagnosis than a general congenital melanocytic nevus.
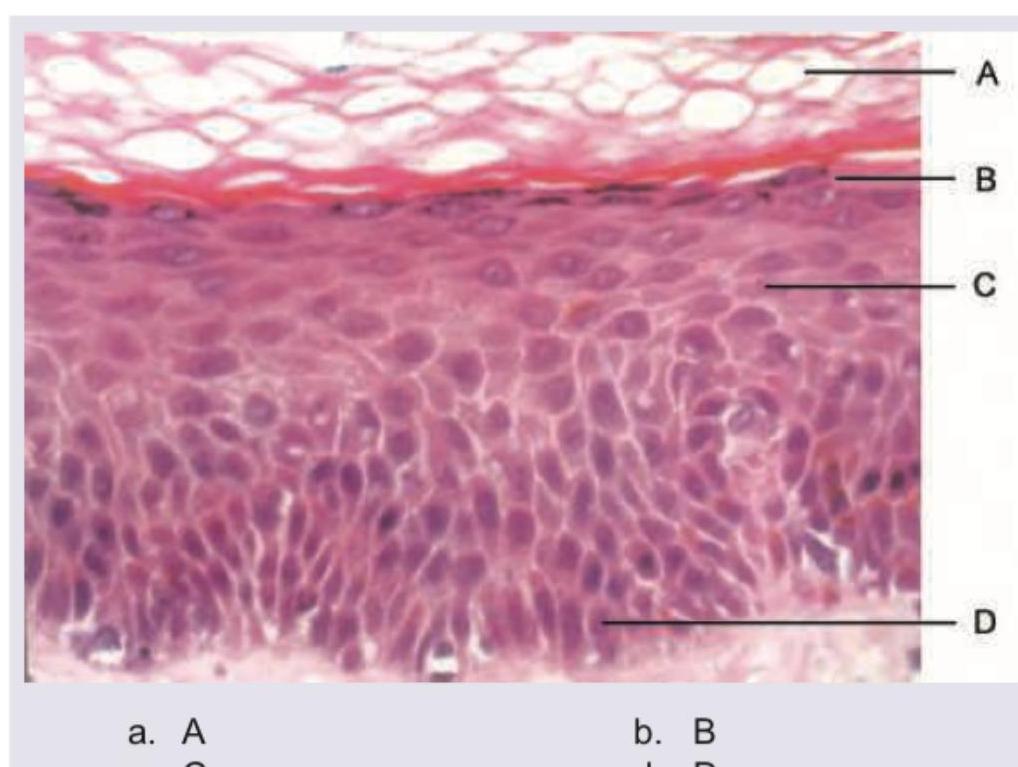
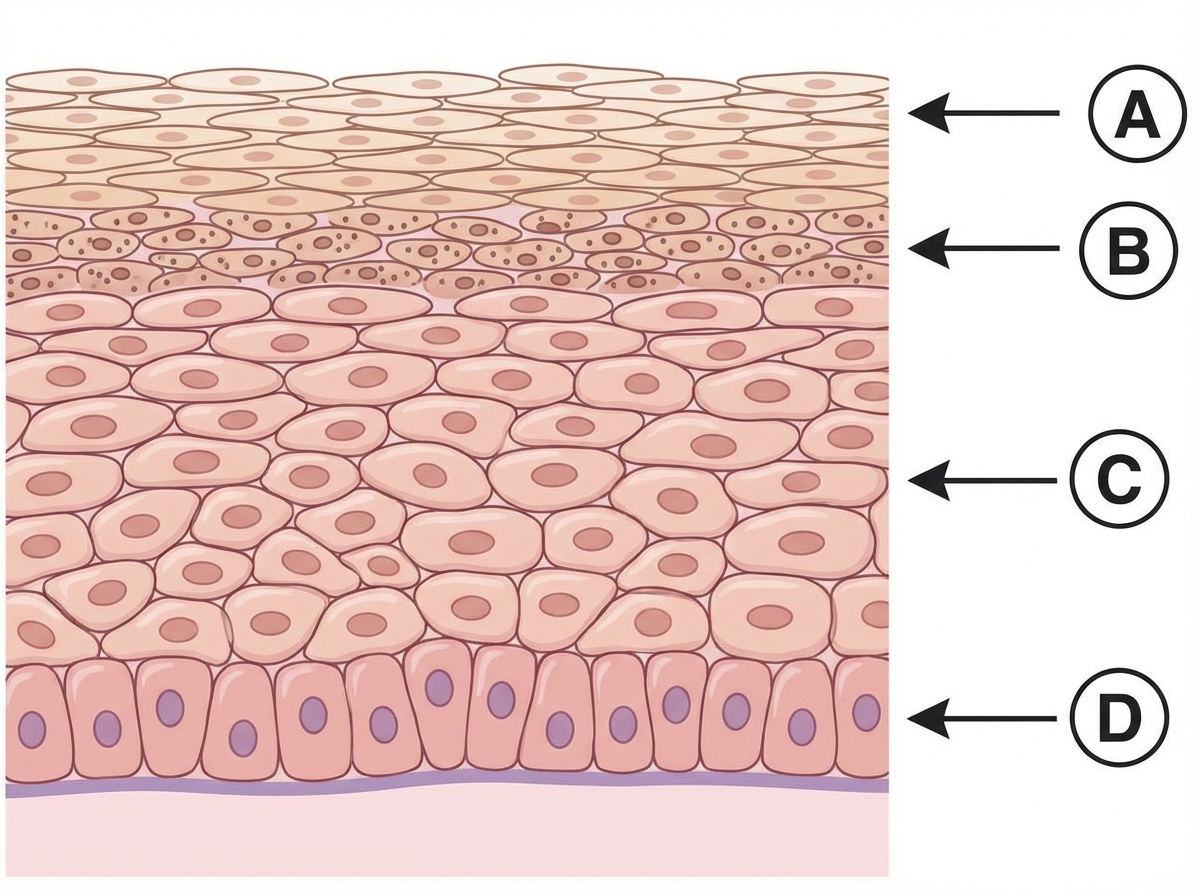
Question 7: Which of the following layers is absent in psoriasis?
- A. A
- B. B (Correct Answer)
- C. C
- D. D
Explanation: ***B*** - The layer labeled 'B' corresponds to the **stratum granulosum (granular layer)** of the epidermis, which is **absent or markedly thinned in areas of parakeratosis** in psoriatic lesions. - The loss/absence of the stratum granulosum in psoriasis is a characteristic histological feature, particularly in regions showing parakeratosis (retention of nuclei in the stratum corneum). - This is considered the classic answer for "which layer is absent in psoriasis" in medical examinations. *A* - The layer labeled 'A' is the **stratum corneum (horny layer)**, which is actually **thickened** in psoriasis (hyperkeratosis) and shows **parakeratosis** (retention of nuclei). - The stratum corneum is not absent but rather abnormal, showing retained nuclei and increased thickness with scaling. *C* - The layer labeled 'C' represents the **stratum spinosum (prickle cell layer)**, which is significantly **thickened (acanthosis)** in psoriasis due to increased keratinocyte proliferation. - Acanthosis (thickening of the spinous layer) is a hallmark feature of psoriasis, not absence of this layer. *D* - The layer labeled 'D' points to the **stratum basale (basal layer)**, which contains actively dividing keratinocytes and is always present in the epidermis. - In psoriasis, the basal keratinocytes show increased proliferation and shortened cell cycle, leading to epidermal hyperplasia, but the layer is never absent.
Question 8: Which of the following layers contains Odland bodies?
- A. A
- B. B (Correct Answer)
- C. C
- D. D
Explanation: ***B*** - The layer indicated by **B** is the **stratum granulosum**, which is characterized by the presence of **keratohyalin granules** and **Odland bodies** (lamellar bodies). - **Odland bodies** are crucial for forming the **epidermal water barrier** as they release lipids and enzymes into the intercellular space. *A* - The layer indicated by **A** is the **stratum corneum**, which consists of dead, flattened keratinocytes. - This layer is primarily involved in protection and does not contain Odland bodies, which are found in deeper layers. *C* - The layer indicated by **C** is the **stratum spinosum**, characterized by many **desmosomes** giving a "spiny" appearance. - While cells in this layer are metabolically active and produce keratin, Odland bodies primarily form and are extruded in the stratum granulosum. *D* - The layer indicated by **D** is the **stratum basale** (or stratum germinativum), the deepest layer of the epidermis. - This layer contains **stem cells** that are constantly dividing to replenish the epidermal layers and is also where melanocytes are located; it does not contain Odland bodies.