All SubjectsAnatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q11
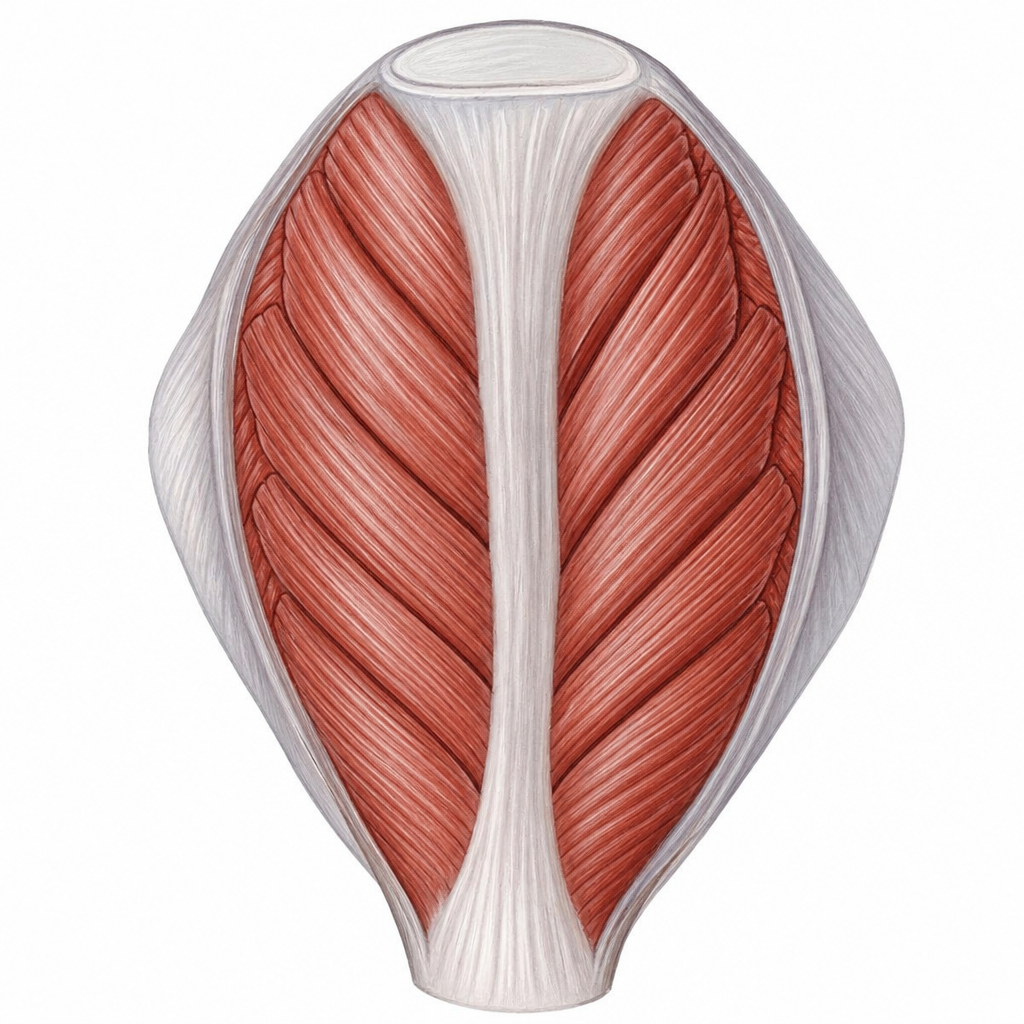
Identify the type of muscle shown in the image.
Q12
Hard palate contains:
Q13
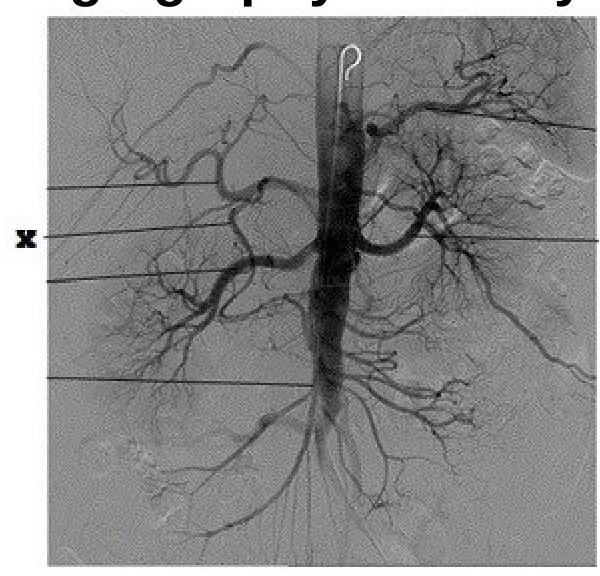
Identify the artery labeled as 'X' in the provided angiography anatomy image.
Q14
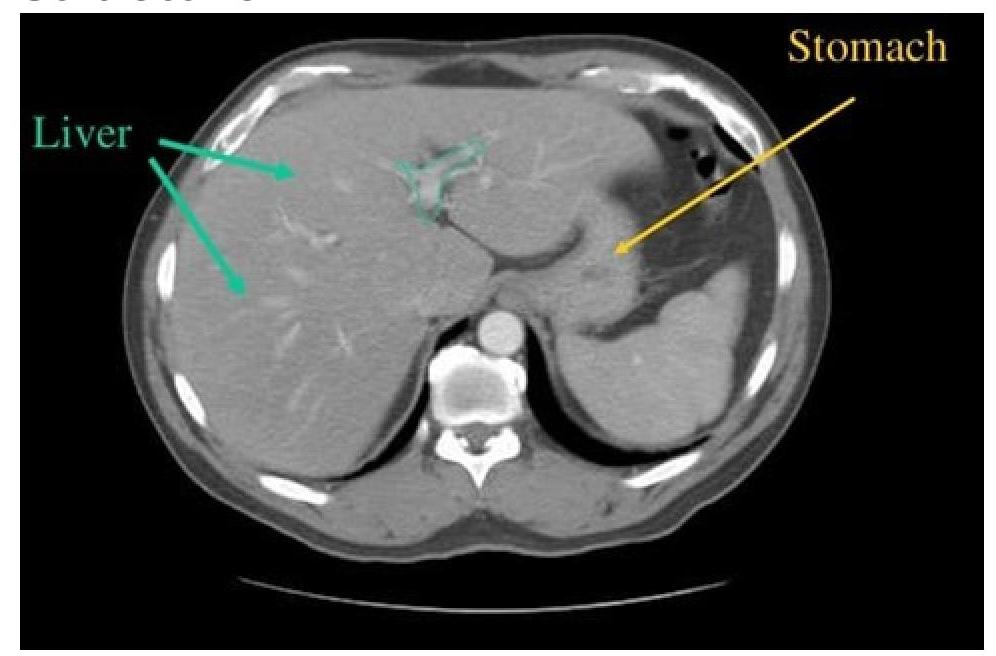
CT scan of abdomen showing a structure branching within the liver. Identify the structure.
Q15
What constitutes the Malpighian layer of skin?
Q16
Which thickened nerve is shown in the image?

Q17
What is the primary function of the deltoid muscle?
Q18
Nerves of pharyngeal arch develop from
Q19
Wallenberg syndrome involves which artery?
Q20
Nasopharyngeal chordoma arises from:-