All SubjectsAnatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Q11
Which mechanism is primarily responsible for the transport of glucose in renal tubular cells?
Q12
Mechanism by which Ach decreases heart rate is by:
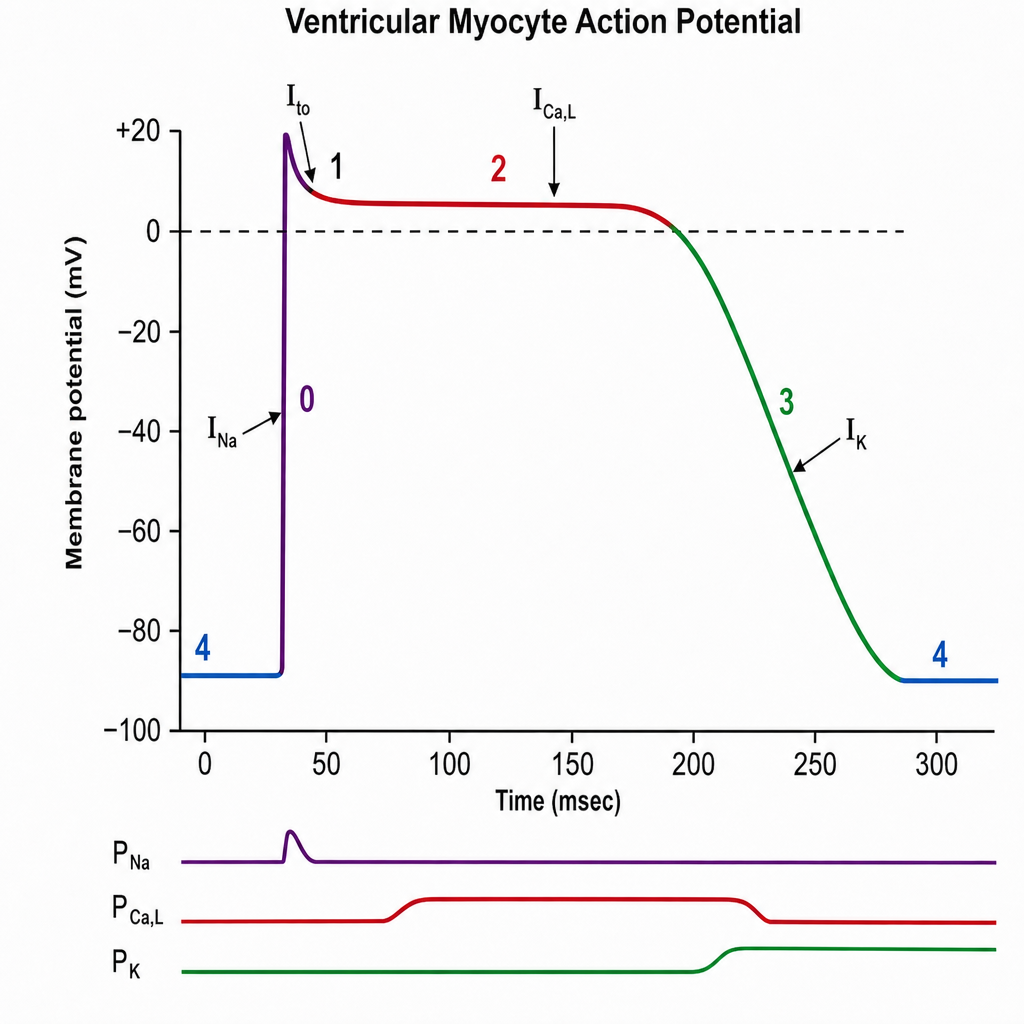
Q13
The plateau phase of this graph is due to:
Q14
What is the normal range for the CSF/plasma glucose ratio?
Q15
Which of the following is most important in sodium and water retention ?
Q16
Peripheral and central chemoreceptors may both contribute to the increased ventilation that occurs as a result of which of the following?
Q17
Which tract is responsible for the loss of proprioception and fine touch?
Q18
Insensible water loss per day is ?
Q19
Ptyalin is secreted by?
Q20
Which type of carbohydrate is absorbed most efficiently from the gastrointestinal tract?