All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Q191
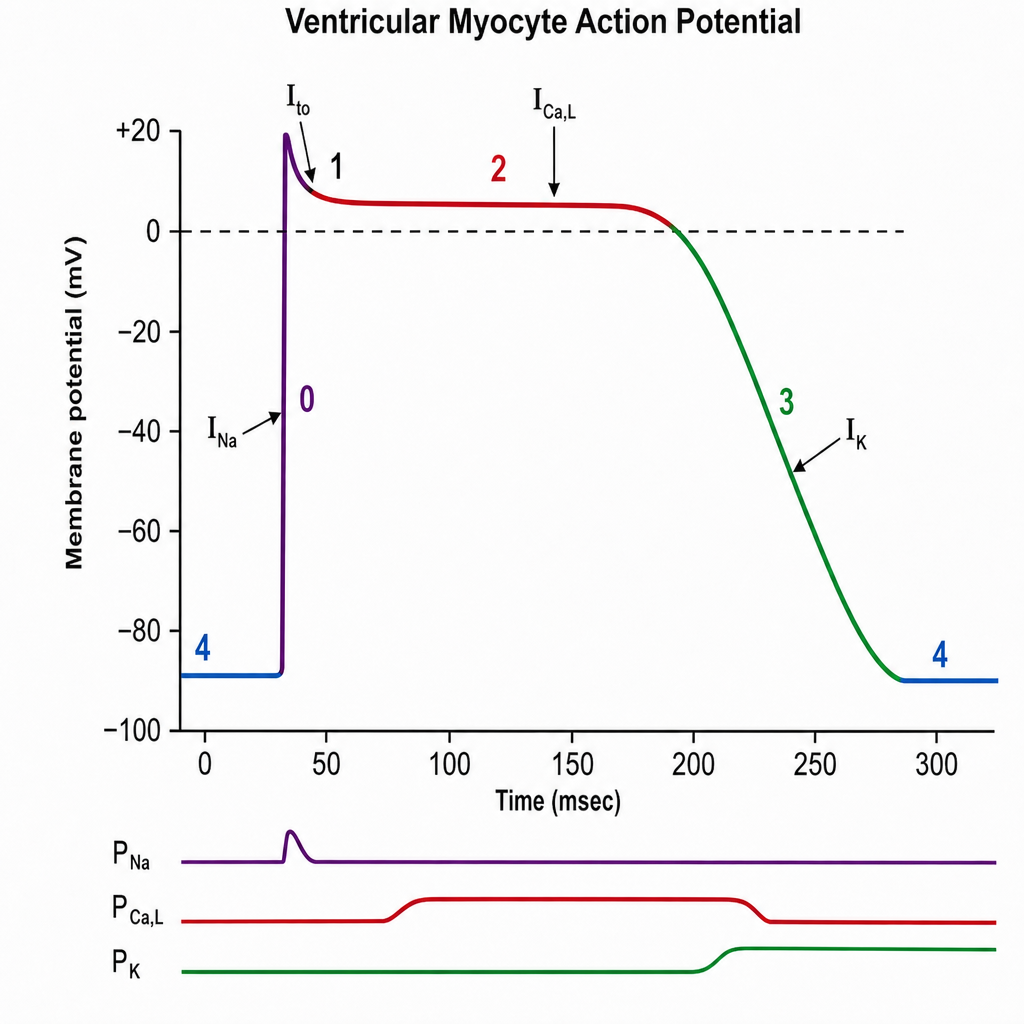
The plateau phase of this graph is due to: