All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Q161
Which of the following is most important in sodium and water retention ?
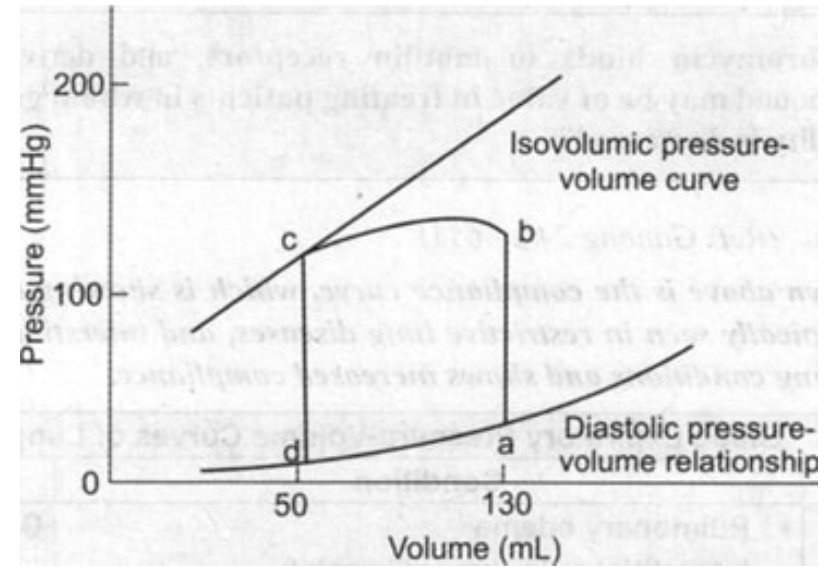
Q162
From the given pressure-volume curve, identify the end-diastolic volume (EDV) and end-systolic volume (ESV), then calculate the ejection fraction using the formula EF = (EDV - ESV)/EDV × 100%.
Q163
What is the process by which water moves from the extracellular space to the intracellular space?
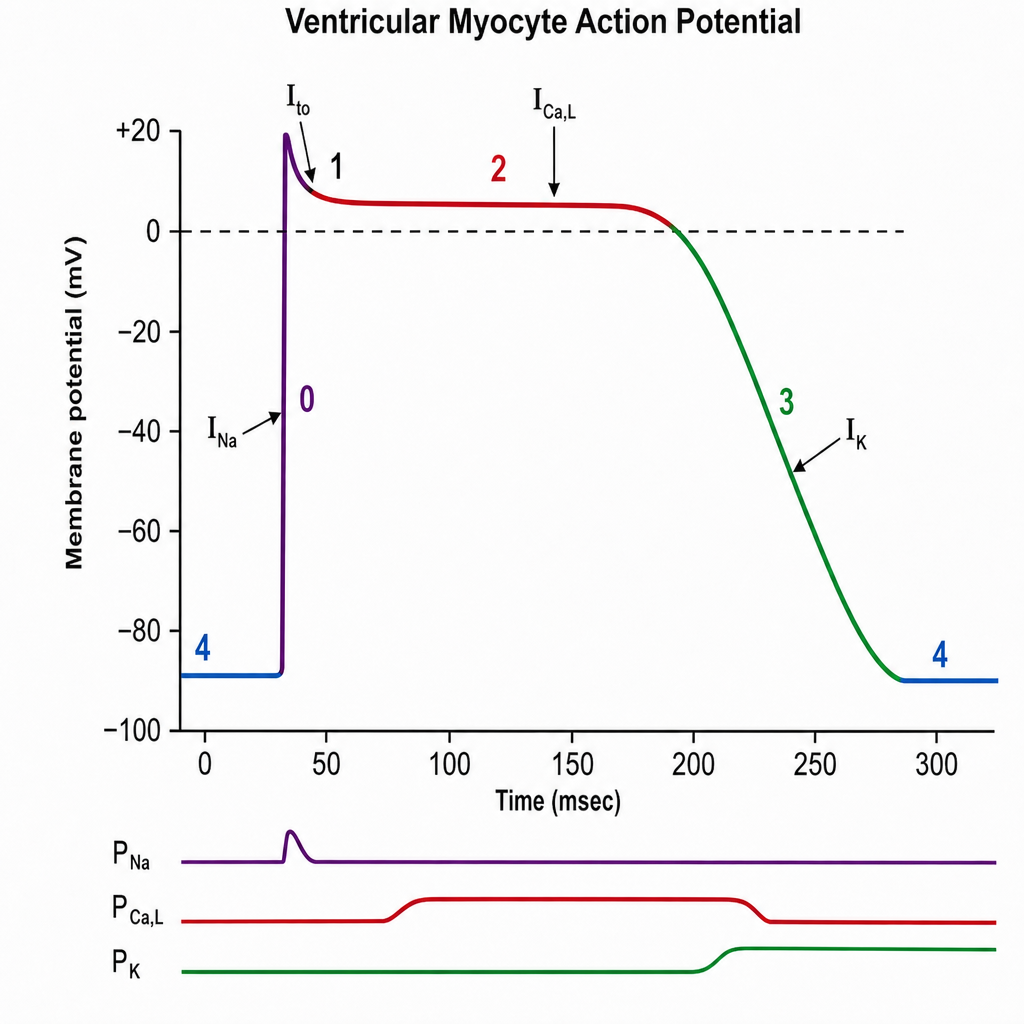
Q164
The plateau phase of this graph is due to: