All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Q1011
Sequestrum is best defined as
Q1012
What is the most common complication associated with carpal tunnel release surgery?
Q1013
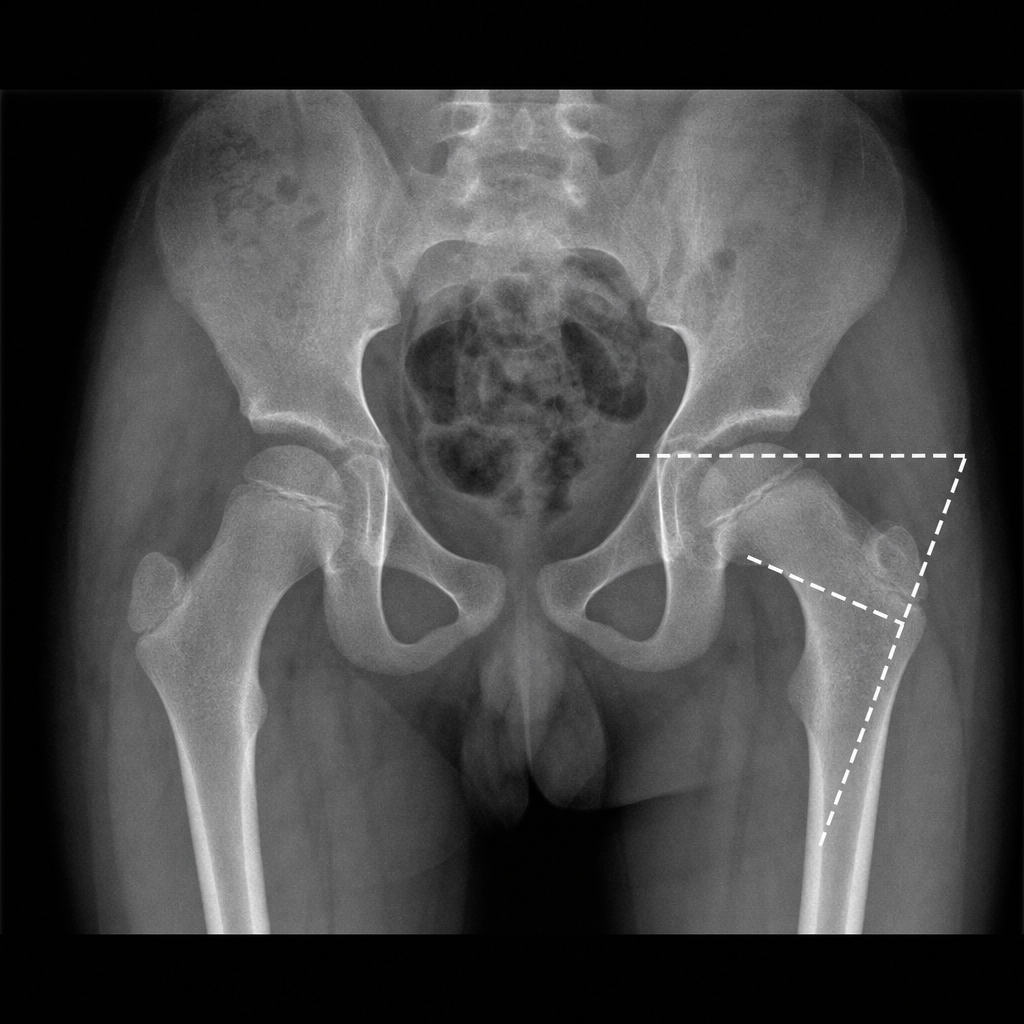
Fairbank triangle is seen in