All (287)Anatomy (26)Anesthesiology (5)Biochemistry (20)Community Medicine (21)Dermatology (10)ENT (11)Forensic Medicine (9)General Medicine (1)Internal Medicine (33)Microbiology (14)Obstetrics and Gynecology (23)Ophthalmology (7)Orthopaedics (5)Pathology (15)Pediatrics (17)Pharmacology (17)Physiology (11)Psychiatry (6)Radiology (11)Surgery (25)
Q181
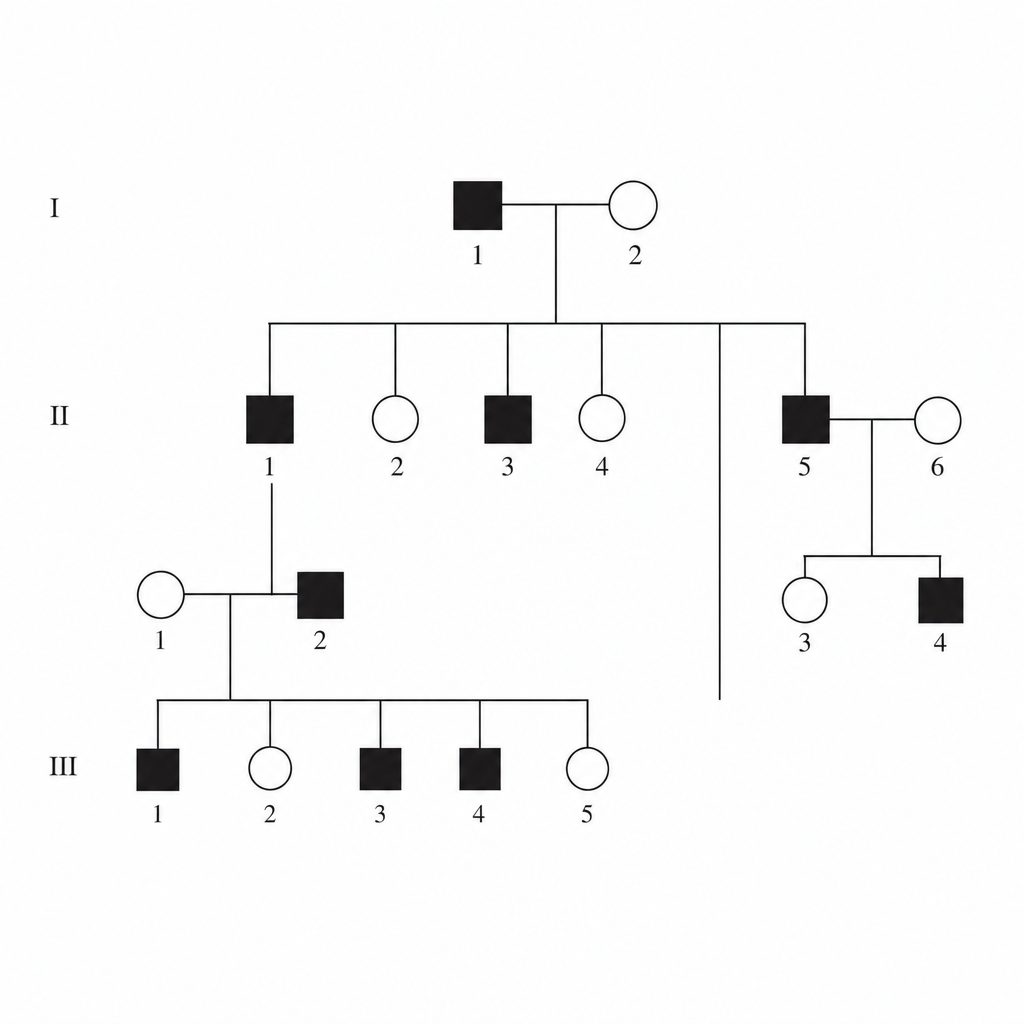
A family pedigree chart is given below. Identify the mode of inheritance of this condition. 
Q182
A family pedigree chart is given below. Identify the mode of inheritance of this condition.