All SubjectsAnatomy (26)Anesthesiology (5)Biochemistry (20)Community Medicine (21)Dermatology (10)ENT (11)Forensic Medicine (9)General Medicine (1)Internal Medicine (33)Microbiology (14)Obstetrics and Gynecology (23)Ophthalmology (7)Orthopaedics (5)Pathology (15)Pediatrics (17)Pharmacology (17)Physiology (11)Psychiatry (6)Radiology (11)Surgery (25)
Q11
Which of the following is not an indication for a cesarean section?
Q12
What is the level of the uterus immediately after delivery?
Q13
Which of the following procedures is done with the instrument shown below?

Q14
Which of the following procedures is done with the instrument shown below? 
Q15
Which of the following is the most common location of implantation in ectopic pregnancy? 
Q16
A young sexually active female patient presented to the outpatient department with complaints of lower abdominal pain, fever, vomiting, and foul-smelling vaginal discharge. On examination, the body temperature is 103 degrees Fahrenheit, pulse rate is 109 per minute and there is abdominal tenderness. Cervical motion tenderness is present on examination. What is the most likely diagnosis?
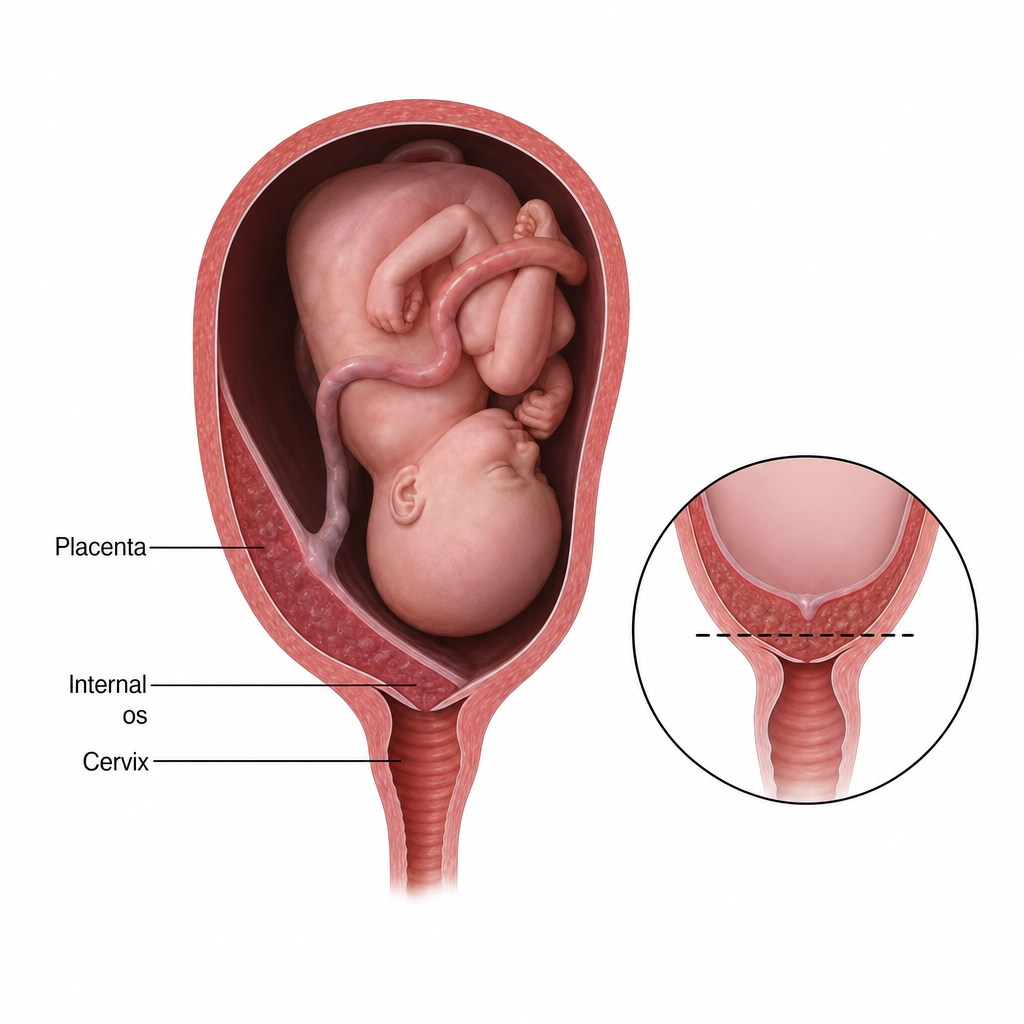
Q17
Identify the given image of the placenta previa. 
Q18
Identify the given image of the placenta previa.
Q19
Identify the following instrument used by obstetricians:
Q20
In which of the following cases is the drug below contraindicated?