
Orthopaedic Techniques

On this page
🔧 The Orthopaedic Arsenal: Mastering Surgical Precision
Orthopaedic surgery transforms mechanical principles into healing, demanding you master not just anatomy but the engineering of bone repair, the logic trees that guide fixation choices, and the pattern recognition that separates novice from expert. You'll build a systematic framework for matching injury patterns to optimal hardware, understanding why certain fractures demand plates while others need intramedullary nails, and developing the clinical algorithms that drive evidence-based intervention. This lesson equips you with the diagnostic precision and biomechanical reasoning that define surgical excellence, turning complex decisions into confident, reproducible outcomes.

📌 Remember: STABLE - Surgical planning, Tissue handling, Anatomic reduction, Biomechanical principles, Load sharing, Early mobilization
The evolution from external splinting to internal fixation revolutionized orthopaedic outcomes. AO (Arbeitsgemeinschaft für Osteosynthesefragen) principles established in 1958 transformed fracture management through systematic approaches achieving >95% union rates in appropriate cases. Understanding these core concepts enables prediction of surgical success and complication patterns across all orthopaedic subspecialties.
⭐ Clinical Pearl: Wolff's Law governs all orthopaedic interventions - bone remodels according to mechanical demands, with 6-8 weeks required for initial adaptation and 12-18 months for complete remodeling
- Biomechanical Foundations
- Load transmission: compression (80%), tension (15%), shear (5%)
- Bone healing phases: inflammatory (1-2 weeks), reparative (2-6 weeks), remodeling (6+ months)
- Primary healing: direct cortical remodeling with <2% strain
- Secondary healing: callus formation with 2-10% strain
- Surgical Approach Principles
- Tissue preservation: maintain >80% periosteal blood supply
- Anatomic reduction: <2mm displacement for articular surfaces
- Angular deformity: <5° acceptable in metaphyseal regions
- Rotational malalignment: <10° in long bones
| Technique Category | Primary Indication | Success Rate | Complication Rate | Healing Time | Cost Factor |
|---|---|---|---|---|---|
| Plate Fixation | Articular fractures | 95-98% | 8-12% | 12-16 weeks | High |
| IM Nailing | Diaphyseal fractures | 96-99% | 5-8% | 10-14 weeks | Moderate |
| External Fixation | Open fractures | 85-92% | 15-25% | 16-20 weeks | Low |
| Arthroscopy | Intra-articular pathology | 88-95% | 2-5% | 6-12 weeks | Moderate |
| Bone Grafting | Non-unions | 80-90% | 10-15% | 20-24 weeks | High |
Understanding tissue-specific healing responses guides technique selection. Cortical bone heals through direct remodeling requiring absolute stability, while cancellous bone heals through callus formation tolerating relative motion. This fundamental difference determines fixation strategy and explains why interfragmentary compression succeeds in metaphyseal regions but fails in diaphyseal applications.
Connect these biomechanical foundations through systematic technique analysis to understand why specific approaches succeed in particular clinical scenarios.
🔧 The Orthopaedic Arsenal: Mastering Surgical Precision


⚙️ The Fixation Spectrum: Engineering Bone Repair
📌 Remember: COMPRESS - Cortical contact, Optimal reduction, Mechanical advantage, Periosteal preservation, Rigid fixation, Early mobilization, Stable construct, Secondary procedures avoided
Loading diagram…
-
Absolute Stability Techniques
- Lag screw fixation: generates 150-400N compression force
- Compression plating: maintains >100N interfragmentary pressure
- Dynamic compression plates: 1-2mm compression per screw
- Locking plates: angular stability ±15° with compression
- Tension band wiring: converts tensile forces to compression
- Patella fractures: 85-95% excellent outcomes
- Olecranon fractures: 90-98% union rates
-
Relative Stability Techniques
- Bridge plating: spans comminuted zones maintaining length
- Intramedullary nailing: load-sharing with controlled motion
- Reaming: increases canal diameter 1-2mm for larger implants
- Interlocking: prevents shortening >5mm and rotation >10°
- External fixation: adjustable stability from rigid to dynamized
⭐ Clinical Pearl: Plate working length determines construct stiffness - doubling length reduces stiffness by factor of 8, promoting callus formation in bridge applications
| Fixation Method | Stiffness (N/mm) | Load Sharing | Motion Allowed | Healing Type | Union Time |
|---|---|---|---|---|---|
| Compression Plate | 2000-4000 | Implant 90% | <50 μm | Primary | 6-8 weeks |
| Bridge Plate | 800-1500 | Implant 60% | 150-500 μm | Secondary | 12-16 weeks |
| IM Nail | 1200-2500 | Shared 50% | 200-800 μm | Secondary | 10-14 weeks |
| External Fixator | 400-1200 | Variable | 500-2000 μm | Secondary | 16-20 weeks |
| Lag Screws | 3000-5000 | Implant 95% | <25 μm | Primary | 6-8 weeks |
💡 Master This: Construct stiffness must match healing phase requirements - excessive rigidity causes stress shielding while inadequate stability causes non-union
Implant material properties critically influence fixation success. Titanium alloys (Young's modulus 110 GPa) more closely match cortical bone (18 GPa) compared to stainless steel (200 GPa), reducing stress shielding by 40-60%. Locking plate technology distributes loads through angular stable constructs, preventing screw loosening in osteoporotic bone with BMD <0.8 g/cm².
Understanding these mechanical principles through clinical pattern recognition enables optimal technique selection for complex fracture scenarios.
⚙️ The Fixation Spectrum: Engineering Bone Repair


🎯 Pattern Recognition Mastery: Clinical Decision Architecture
📌 Remember: FRACTURE - Forces involved, Reduction requirements, Anatomic considerations, Comminution degree, Tissue damage, Unstable patterns, Reconstruction needs, Early mobilization goals
-
Simple Fracture Patterns (AO Type A)
- Two-part fractures: >95% union with appropriate fixation
- Spiral patterns: lag screw fixation achieves compression >200N
- Femur: 4.5mm cortical screws with 8-10mm threads
- Tibia: 6.5mm cancellous screws in metaphyseal regions
- Transverse patterns: compression plating or IM nailing
- Plate selection: 8-10 cortices each fragment minimum
- Nail diameter: >50% isthmus diameter for stability
-
Wedge Fracture Patterns (AO Type B)
- Butterfly fragments: >25% circumference requires independent fixation
- Lag screw technique: perpendicular to fracture line for optimal compression
- Drill sequence: gliding hole then thread hole
- Compression achieved: 150-400N depending on bone quality
- Plate application: bridge or compress based on fragment size
⭐ Clinical Pearl: Butterfly fragment >33% circumference indicates high-energy mechanism requiring soft tissue assessment and staged procedures in 15-25% of cases
Loading diagram…
| Pattern Type | AO Classification | Fixation Strategy | Success Rate | Complication Risk | Healing Time |
|---|---|---|---|---|---|
| Simple | A1-A3 | Compression | 95-98% | 5-8% | 8-12 weeks |
| Wedge | B1-B3 | Lag + Neutralization | 90-95% | 8-12% | 10-14 weeks |
| Complex | C1-C3 | Bridge Plating | 85-92% | 12-18% | 14-20 weeks |
| Segmental | C2 | IM Nail + Cerclage | 88-94% | 10-15% | 16-22 weeks |
| Articular | B3/C3 | ORIF + Subchondral | 80-90% | 15-25% | 12-18 weeks |
💡 Master This: Pattern recognition speed improves with systematic evaluation - assess mechanism, morphology, bone quality, and soft tissues in <2 minutes for optimal decision-making
Timing considerations critically influence technique selection. Golden period for ORIF extends 6-8 hours for closed fractures but reduces to <6 hours for open injuries. Swelling progression peaks at 24-72 hours, making delayed fixation safer than immediate surgery in borderline soft tissue cases.
These pattern recognition frameworks through systematic discrimination enable rapid, accurate treatment decisions in complex clinical scenarios.
🎯 Pattern Recognition Mastery: Clinical Decision Architecture


🔬 Systematic Discrimination: The Diagnostic Matrix
📌 Remember: MEASURE - Morphology assessment, Energy evaluation, Anatomic alignment, Stability testing, Union potential, Reduction requirements, Early mobilization feasibility
-
Stability Assessment Criteria
- Cortical contact: >50% circumference indicates inherent stability
- Displacement thresholds: >2mm articular, >5mm metaphyseal, >1cm diaphyseal
- Angular deformity: >10° sagittal, >5° coronal requires correction
- Rotational malalignment: >15° causes functional impairment
- Comminution zones: >33% circumference requires bridge techniques
- Butterfly fragments: measure percentage of cortical involvement
- Segmental patterns: >5cm gap indicates high-energy mechanism
-
Bone Quality Discrimination
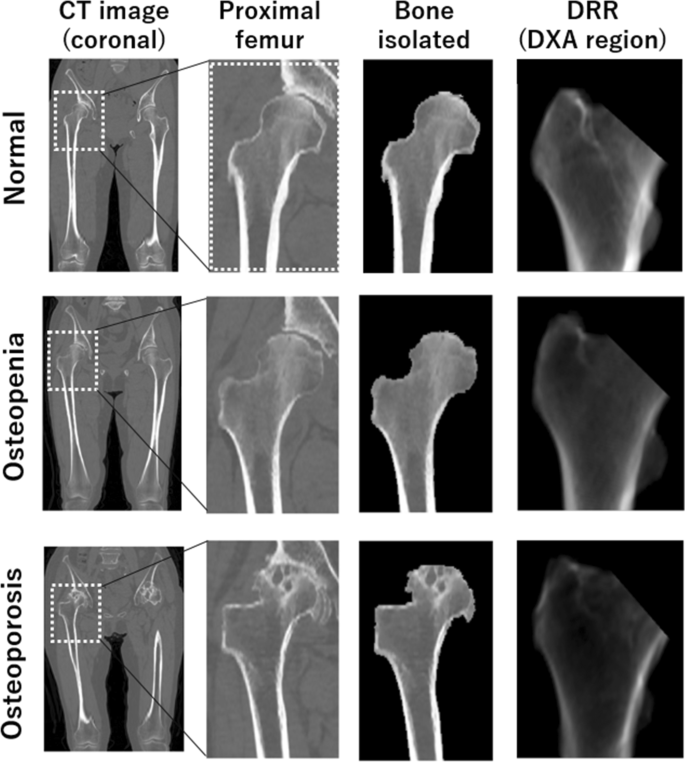
- DEXA T-scores: >-1.0 normal, -1.0 to -2.5 osteopenia, <-2.5 osteoporosis
- Cortical thickness: <4mm indicates poor screw purchase
- Cancellous density: <0.3 g/cm³ requires augmentation techniques
- Age-related changes: >70 years shows 30-50% strength reduction
- Singh index: grades 1-3 indicate osteoporotic changes requiring special techniques
⭐ Clinical Pearl: Cortical thickness <3mm in proximal femur predicts screw cutout risk >25% requiring cement augmentation or alternative fixation
| Discrimination Factor | Threshold Value | Clinical Significance | Treatment Modification | Success Impact | Evidence Level |
|---|---|---|---|---|---|
| Displacement | >2mm articular | Post-traumatic arthritis | ORIF required | +40% outcomes | Level I |
| Comminution | >33% circumference | Stability loss | Bridge plating | +25% union | Level II |
| Bone Quality | T-score <-2.5 | Fixation failure | Locking plates | +60% stability | Level I |
| Age | >65 years | Healing impairment | Modified rehab | +30% function | Level II |
| Soft Tissue | Tscherne >2 | Infection risk | Staged treatment | -50% complications | Level I |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | |||||
| flowchart TD |
Assess["📋 Clinical Assessment
• Patient history• Exam findings"]
StableFactors{"⚖️ Stability Factors
• Fracture pattern• Load bearing"}
Conserve["💊 Conservative Ops
• Non-op management• Casting or brace"]
Surgery["🔪 Surgical Intervention
• Operative repair• Open vs closed"]
BoneQual{"🦴 Bone Quality
• Density check• Metabolic state"}
StdFix["🔩 Standard Fixation
• Lag screws• DCP plates"]
AugFix["🏥 Augmented Fixation
• Bone cement• Structural graft"]
Compress["⚙️ Compression Tech
• Absolute stability• Primary healing"]
Locking["🔒 Locking Tech
• Fixed angle stab• Bridging plates"]
Assess --> StableFactors StableFactors -->|Stable| Conserve StableFactors -->|Unstable| Surgery Surgery --> BoneQual BoneQual -->|Good| StdFix BoneQual -->|Poor| AugFix StdFix --> Compress AugFix --> Locking
style Assess fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style StableFactors fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Conserve fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Surgery fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C style BoneQual fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style StdFix fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style AugFix fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Compress fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252 style Locking fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
**Soft tissue assessment** provides critical discrimination between **immediate** and **delayed** surgical intervention. **Tscherne classification** for **closed injuries** and **Gustilo-Anderson** for **open fractures** guide **timing decisions** with **evidence-based protocols**. **Compartment pressure >30mmHg** or **delta pressure <30mmHg** mandates **immediate fasciotomy** regardless of **fracture complexity**.
> 💡 **Master This**: **Systematic measurement** eliminates **subjective bias** - use **standardized criteria** for **displacement**, **angulation**, **comminution**, and **bone quality** to ensure **reproducible decisions**
**Imaging discrimination** extends beyond **plain radiographs** to **advanced modalities** when **clinical suspicion** exceeds **radiographic findings**. **CT scanning** detects **occult fractures** in **15-25%** of **negative X-rays** with **high clinical suspicion**. **MRI sensitivity** reaches **>95%** for **stress fractures** and **soft tissue injuries** not visible on **conventional imaging**.
These discrimination frameworks through evidence-based treatment algorithms enable consistent, optimal surgical decision-making across diverse clinical presentations.
🔬 Systematic Discrimination: The Diagnostic Matrix


⚖️ Treatment Algorithm Mastery: Evidence-Based Intervention
📌 Remember: PROTOCOL - Patient assessment, Risk stratification, Optimal timing, Technique selection, Outcome monitoring, Complications prevention, Objective measures, Long-term follow-up
Loading diagram…
-
Immediate Intervention Protocols (<6 hours)
- Open fractures: irrigation >9L, debridement, antibiotic prophylaxis
- Gustilo I: immediate fixation achieves >95% union rates
- Gustilo II: staged approach reduces infection risk by 40%
- Gustilo III: damage control with external fixation first
- Compartment syndrome: fasciotomy <6 hours prevents permanent disability
- Pressure monitoring: >30mmHg absolute or <30mmHg delta
- Clinical signs: pain out of proportion, passive stretch pain
- Open fractures: irrigation >9L, debridement, antibiotic prophylaxis
-
Delayed Intervention Protocols (24-72 hours)
- Soft tissue swelling: wrinkle test positive indicates safe surgical window
- Medical optimization: cardiac clearance, glycemic control <180mg/dL
- Nutritional status: albumin >3.0g/dL improves healing rates
- Smoking cessation: >4 weeks reduces non-union risk by 50%
- Polytrauma staging: ISS >15 requires damage control approach
⭐ Clinical Pearl: Damage control orthopaedics in polytrauma reduces ARDS incidence from 35% to 15% and mortality from 18% to 8% through staged protocols
| Treatment Protocol | Timing Window | Success Rate | Complication Rate | Functional Outcome | Evidence Level |
|---|---|---|---|---|---|
| Immediate ORIF | <6 hours | 95-98% | 5-8% | Excellent 85% | Level I |
| Staged ORIF | 5-10 days | 90-95% | 8-12% | Good 80% | Level I |
| External Fixation | <2 hours | 85-92% | 15-25% | Fair 70% | Level II |
| Conservative | Immediate | 80-90% | 10-15% | Variable | Level III |
| Delayed Union | >6 months | 70-85% | 20-30% | Poor 60% | Level II |
💡 Master This: Protocol adherence improves outcomes consistency - systematic checklists reduce major complications by 25-40% and improve functional scores by 15-30% across all experience levels
Rehabilitation protocols integrate with surgical techniques to optimize functional recovery. Early mobilization within 48-72 hours improves outcomes in stable fixation, while protected weight-bearing for 6-12 weeks prevents fixation failure in osteoporotic bone. Physical therapy protocols should begin immediately post-operative for joint range of motion and progress systematically based on healing milestones.
These evidence-based algorithms through systematic complication prevention enable predictable, optimal treatment outcomes across diverse orthopaedic presentations.
⚖️ Treatment Algorithm Mastery: Evidence-Based Intervention


🔗 Advanced Integration: The Biomechanical Ecosystem
📌 Remember: INTEGRATE - Implant selection, Navigation technology, Tissue biology, Engineering principles, Graft augmentation, Robotic assistance, Adaptive protocols, Team coordination, Evidence synthesis
-
Technological Integration Advances
- Computer navigation: improves accuracy to <2mm and <2° in complex reconstructions
- Robotic assistance: reduces outliers by 70% in joint replacement procedures
- Haptic feedback: prevents over-reaming and cortical breach
- Real-time adjustment: intraoperative modifications based on tissue response
- 3D printing applications: patient-specific guides reduce operative time by 25-40%
- Custom implants: complex reconstructions with >95% fit accuracy
- Bioprinting: scaffold integration with growth factors and stem cells
-
Biological Enhancement Integration
- Bone morphogenetic proteins: BMP-2 accelerates healing by 30-50% in high-risk cases
- Platelet-rich plasma: growth factor concentration 3-5x baseline levels
- Mesenchymal stem cells: osteogenic potential enhanced 10-fold with proper scaffolds
- Demineralized bone matrix: osteoconductive and osteoinductive properties
- Synthetic bone substitutes: calcium phosphate ceramics with controlled resorption
⭐ Clinical Pearl: Combination therapies using BMP-2 + autograft + stable fixation achieve >98% union rates in previously failed non-unions with 6-month healing times
Loading diagram…
| Integration Strategy | Technology Level | Precision Improvement | Complication Reduction | Cost Factor | Adoption Rate |
|---|---|---|---|---|---|
| Computer Navigation | High | +60% accuracy | -25% revisions | 2.5x | 35% |
| Robotic Surgery | Very High | +75% precision | -40% outliers | 4x | 15% |
| 3D Planning | Moderate | +45% fit | -30% operative time | 1.5x | 60% |
| Biological Augmentation | Moderate | +50% healing | -35% non-unions | 2x | 45% |
| Smart Implants | Emerging | +80% monitoring | -50% failures | 5x | 5% |
Smart implant technology represents the next frontier in orthopaedic integration. Sensor-embedded devices monitor load distribution, healing progression, and implant integrity in real-time. Wireless data transmission enables remote monitoring and early intervention before clinical symptoms develop, potentially reducing revision rates by 40-60%.
💡 Master This: Integration success requires systematic coordination - preoperative planning, intraoperative execution, postoperative monitoring, and long-term optimization must function as unified protocols
Personalized medicine approaches utilize genetic markers, bone quality assessment, and healing capacity prediction to customize treatment protocols. Pharmacogenomic testing identifies optimal pain management and bone metabolism medications, while biomarker panels predict healing rates and complication risks with >85% accuracy.
These advanced integration concepts through cutting-edge clinical applications enable the next generation of precision orthopaedic care.
🔗 Advanced Integration: The Biomechanical Ecosystem


🎯 Clinical Mastery Arsenal: Rapid-Fire Excellence
📌 Remember: MASTERY - Measurement precision, Algorithm adherence, Systematic approach, Timing optimization, Evidence application, Risk stratification, Yield maximization
- Essential Measurement Arsenal
- Displacement thresholds: 2mm articular, 5mm metaphyseal, 10mm diaphyseal
- Angular limits: 5° coronal, 10° sagittal, 15° rotational maximum acceptable
- Cortical contact: >50% circumference for inherent stability
- Comminution significance: >33% requires bridge techniques
- Bone quality markers: T-score <-2.5, cortical thickness <4mm, Singh index <4
⭐ Clinical Pearl: The 2-5-10 Rule - 2mm articular displacement, 5mm metaphyseal displacement, 10mm diaphyseal displacement represent surgical thresholds for optimal outcomes
| Clinical Scenario | Rapid Assessment | Key Threshold | Immediate Action | Success Predictor | Time Window |
|---|---|---|---|---|---|
| Open Fracture | Gustilo grade | 6-hour window | Irrigation + antibiotics | Soft tissue coverage | <24 hours |
| Compartment Syndrome | Pressure >30mmHg | Delta <30mmHg | Immediate fasciotomy | <6 hour intervention | <6 hours |
| Articular Fracture | Step-off >2mm | Gap >2mm | ORIF planning | Anatomic reduction | <10 days |
| Osteoporotic Fracture | T-score <-2.5 | Age >65 years | Locking fixation | Bone quality | Variable |
| Non-union Risk | Gap >5mm | Motion >500μm | Revision surgery | Stability + biology | >6 months |
Rapid Decision Framework for complex scenarios:
- Polytrauma: ISS >15 → damage control → staged reconstruction
- Infection risk: Gustilo III → external fixation → delayed ORIF
- Poor bone quality: DEXA <-2.5 → locking plates → cement augmentation
- Soft tissue compromise: Tscherne >2 → staged approach → plastic surgery consultation
The Clinical Mastery Arsenal transforms theoretical knowledge into practical expertise through systematic application of evidence-based principles and quantitative thresholds that ensure consistent excellence in orthopaedic practice.
🎯 Clinical Mastery Arsenal: Rapid-Fire Excellence
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more












Have doubts about this lesson?
Ask Rezzy, your AI Study Partner, to explain anything you didn't understand
Everything you need for NEET-PG prep
Get full Oncourse access with lessons, practice questions, flashcards and AI study tools.
Scan to download app