Back
How to Study Surgery for USMLE Step 2 CK: High-Yield Topics, Surgical Emergencies and Exam Strategy (2026)
Master USMLE Step 2 CK surgery with this comprehensive guide covering high-yield topics, surgical emergencies, trauma protocols, and exam strategy for 2026.
How to Study Surgery for USMLE Step 2 CK: High-Yield Topics, Surgical Emergencies and Exam Strategy (2026)
You are probably thinking surgery is just another clerkship to survive. Step 2 CK has 318 questions. Surgery comprises 15–20% of them — that is 48-64 questions, more than psychiatry and pediatrics combined. Yet most USMLE guides treat surgery as a footnote after internal medicine.
This is wrong. Surgery questions on Step 2 CK are decision-heavy, algorithm-driven, and unforgiving. Miss the management pathway for cardiac tamponade or AAA rupture, and there is no partial credit. The good news? Surgery follows predictable patterns once you understand what the exam actually tests.
Step 2 CK doesnt care if you can perform a cholecystectomy. It tests whether you know when to order a HIDA scan versus going straight to the OR. The mindset shift from "how to operate" to "when to operate" changes everything.
What Makes Surgery Different on Step 2 CK
Surgery questions test management decisions under pressure. Every vignette comes down to a branch point: stable patient → image first, unstable patient → OR immediately. The exam loves testing your ability to triage, recognize surgical emergencies, and manage post-operative complications.
Unlike internal medicine where you can hedge with "monitor closely," surgery demands binary decisions. Either the patient needs emergency surgery or they dont. Either those are hard signs of vascular injury or soft signs. This precision makes surgery both challenging and predictable.
Surgery accounts for roughly 15–20% of Step 2 CK, making it the third-largest clinical topic after internal medicine and psychiatry. For IMGs who may have limited surgical exposure, this percentage often catches test-takers off guard. The key is understanding that surgical knowledge on Step 2 CK focuses heavily on emergency presentations and post-operative management rather than operative techniques.
The Core Mindset: Stability Rules Everything
Every surgery question boils down to patient stability. Here is the decision tree that runs through 80% of surgical scenarios:
Unstable patient (hypotensive, altered mental status, active bleeding):
Skip imaging
Go directly to OR
Exceptions are rare and explicitly stated
Stable patient (normal vitals, alert, localized pain):
Image first (CT, ultrasound, X-ray)
Then decide surgical vs. conservative management
Time allows for workup
This stability rule applies to trauma, acute abdomen, vascular emergencies, and post-op complications. Master this framework, and you have solved the majority of surgery questions before reading the answer choices.
High-Yield Surgery Topics by System
Trauma Management (ATLS Approach)
Trauma follows the primary survey: ABCDE. Step 2 CK loves testing your ability to prioritize life-threatening injuries and apply ATLS protocols.
Chest Trauma:
Tension pneumothorax: Immediate needle decompression, no time for chest X-ray
Massive hemothorax: >1500 mL immediate output or >200 mL/hour ongoing → thoracotomy
Cardiac tamponade: Beck triad (elevated JVP, hypotension, muffled heart sounds) → pericardiocentesis
Pulmonary contusion: Supportive care, avoid fluid overload
Abdominal Trauma:
Blunt trauma with unstable vitals: FAST exam → OR if positive
Penetrating abdominal trauma: Anterior abdominal wall penetration → exploratory laparotomy
Retroperitoneal hematoma: Stable patient → CT scan, unstable → OR
Vascular Injury Signs:
Understanding hard versus soft signs of vascular injury is high-yield for Step 2 CK:
Hard signs (immediate surgery):
Active hemorrhage
Absent pulse
Expanding hematoma
Bruit or thrill
Hard neurologic deficit
Soft signs (CTA first):
Small hematoma
Proximity to major vessel
Diminished pulse
Peripheral nerve injury
When you encounter trauma scenarios, Oncourse AI's adaptive question engine identifies knowledge gaps in ATLS protocols and serves targeted practice until these decision trees become automatic.
Acute Abdomen Algorithms
Acute abdomen questions test your ability to differentiate surgical emergencies from medical management. The key is recognizing patterns and applying the right diagnostic sequence.
Appendicitis:
Right lower quadrant pain + migration + fever
CT scan for diagnosis in stable patients
McBurney point tenderness, Rovsing sign, psoas sign
Perforated appendicitis: broader antibiotic coverage
Bowel Obstruction:
Small bowel: cramping pain, vomiting, minimal abdominal distension
Large bowel: gradual onset, significant distension, late vomiting
Complete obstruction with strangulation → immediate surgery
Partial obstruction → trial of conservative management
Abdominal Aortic Aneurysm (AAA):
Classic triad: abdominal/back pain + hypotension + pulsatile mass
Ruptured AAA → OR immediately, no imaging
Stable AAA >5.5 cm → elective repair
<5.5 cm → surveillance
Mesenteric Ischemia:
Acute onset severe abdominal pain out of proportion to exam
Pain greater than physical findings
Risk factors: atrial fibrillation, recent MI
CT angiography for diagnosis, immediate surgery for confirmed ischemia
Post-Operative Complications Timeline
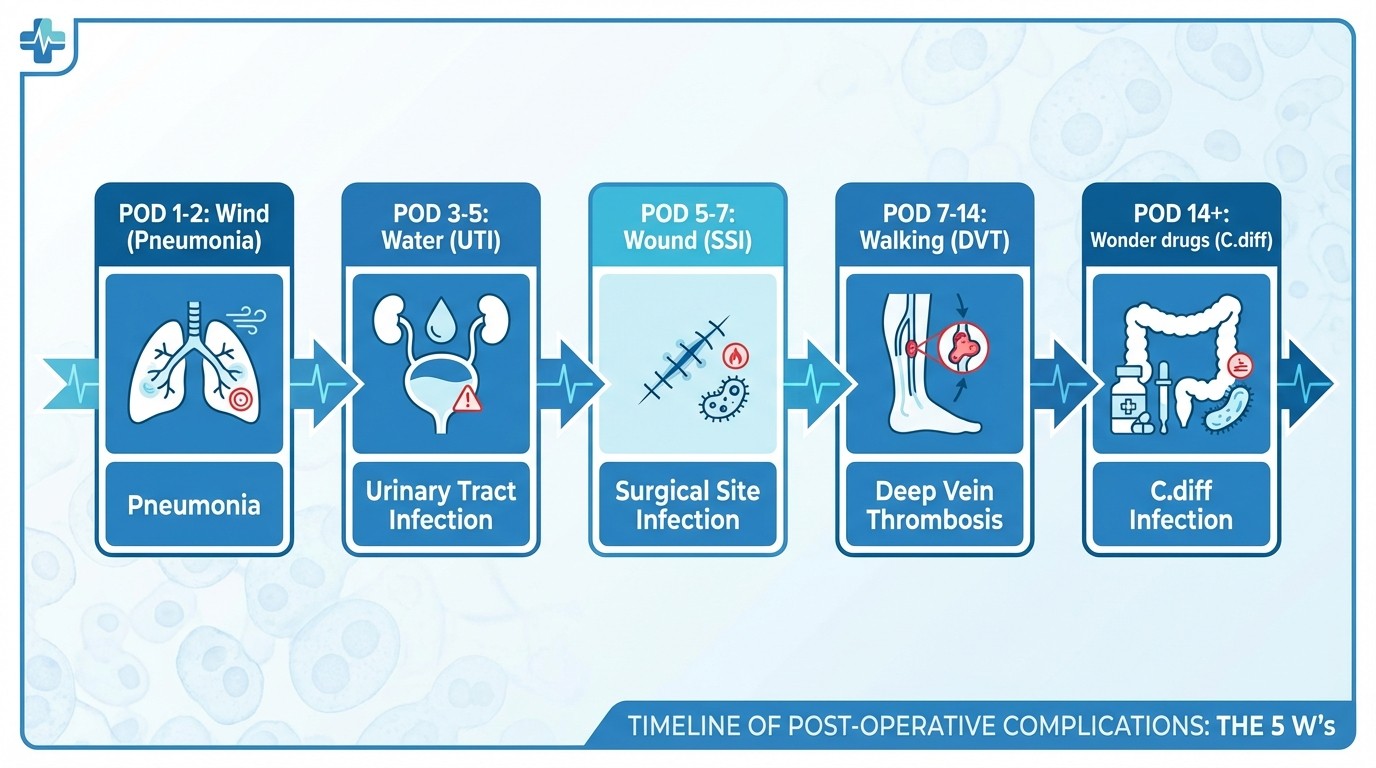
Post-operative fever follows a predictable timeline that Step 2 CK tests repeatedly. The mnemonic "Wind, Water, Wound, Walking, Wonder drugs" maps to specific timeframes:
POD 1-2 (Wind): Pneumonia, atelectasis POD 3-5 (Water): UTI, line infections POD 5-7 (Wound): Surgical site infection POD 7-14 (Walking): DVT, pulmonary embolism POD 14+ (Wonder drugs): C. diff colitis, candidemia Anastomotic Leak:
GI surgery patients with fever + abdominal pain after POD 5
CT with oral contrast shows extravasation
Requires reoperation and diversion
Urinary Retention:
Common after general anesthesia + bladder instrumentation
Bladder scan >400 mL → straight catheterization
Persistent retention → Foley catheter
Oncourse's spaced repetition system surfaces these post-op complication patterns at optimal intervals, preventing the common mistake of confusing timeline-specific complications during high-pressure exam situations.
Vascular Emergencies
Vascular emergencies demand immediate recognition and appropriate intervention. Step 2 CK focuses on acute presentations where time-to-treatment determines outcomes.
Acute Limb Ischemia (6 Ps):
Pain, Pallor, Pulselessness, Paresthesias, Paralysis, Poikilothermia
<6 hours: embolectomy or thrombolysis possible
>6 hours: amputation risk increases dramatically
Always check for atrial fibrillation as embolic source
Aortic Dissection:
Type A (ascending aorta): immediate surgery
Type B (descending aorta): medical management unless complications
CT angiography for diagnosis in stable patients
Control blood pressure with esmolol + nicardipine
Ruptured AAA:
Classic triad present in <50% of cases
Hypotensive patient with abdominal pain → OR immediately
No time for CT scan in unstable patients
EVAR vs. open repair based on anatomy and stability
Endocrine and GI Surgery Essentials
Thyroid Nodules:
TSH first: suppressed → radioiodine uptake scan
Normal/elevated TSH → FNA biopsy
FNA indications: >1 cm nodule with suspicious features
Suspicious features: microcalcifications, hypoechoic, irregular borders
Crohn Disease Surgical Indications:
Obstruction unresponsive to medical therapy
Perforation or abscess formation
Severe bleeding
Malignancy or high-grade dysplasia
Growth retardation in pediatric patients
When studying endocrine surgery decision trees, every question explanation on Oncourse breaks down the clinical reasoning behind each diagnostic step, mirroring exactly how Step 2 CK vignettes are constructed.
Step 2 CK Surgery Study Strategy
During Surgery Clerkship
Week 1-2: Foundation Building
Focus on surgical emergencies and trauma protocols
Master the stability rule and hard vs. soft signs
Complete trauma surgery question sets daily
Week 3-4: Systems Integration
Acute abdomen workups and surgical indications
Post-operative complication recognition and management
Practice vascular emergency algorithms
Week 5-6: Advanced Topics
Endocrine surgery decision trees
Complex GI surgery scenarios
Integrate surgery with other clerkships (anesthesia, radiology)
Week 7-8: Exam Preparation
High-yield review and weak area identification
Timed practice sets focusing on decision speed
Post-operative care and complication management
After Surgery Clerkship
Maintenance Phase (Ongoing):
20-30 surgery questions weekly to maintain knowledge
Focus on commonly missed topics identified through practice
Review surgical emergencies monthly using active recall
Final 4 Weeks Before Step 2 CK:
Surgery-focused question blocks 3x per week
Review trauma algorithms and post-op timelines
Practice surgical decision-making under time pressure
UWorld Surgery Block Strategy
Approach surgery questions systematically:
1. Read the vignette for stability markers first
2. Identify the system involved (trauma, abdomen, vascular)
3. Apply the appropriate algorithm (ATLS, acute abdomen workup)
4. Choose the next best step based on stability and timeframe
When you miss surgery questions, the pattern usually involves:
Misreading stability cues
Confusing hard vs. soft signs
Wrong post-operative complication timeline
Skipping necessary imaging in stable patients
For trauma scenarios specifically, practice with trauma surgery lessons that walk through ATLS protocols step-by-step.
Common Surgery Study Mistakes to Avoid
Mistake 1: Studying Anatomy Instead of Management
Step 2 CK doesnt test anatomical landmarks or surgical approaches. Focus on when to operate, not how to operate. Skip detailed anatomy review in favor of decision algorithms.
Mistake 2: Ignoring Post-Operative Complications
Post-op management comprises 30% of surgery questions on Step 2 CK. The Wind/Water/Wound/Walking timeline is more high-yield than most operative indications.
Mistake 3: Overthinking Trauma Questions
ATLS protocols exist to simplify complex scenarios. Trust the algorithm: ABCs, primary survey, FAST exam, then definitive management. Dont look for zebras in trauma.
Mistake 4: Confusing Imaging Priorities
Stable patients get imaging first. Unstable patients go to the OR. This rule has very few exceptions, and the exam will make exceptions obvious when they exist.
Mistake 5: Neglecting Vascular Emergencies
Hard vs. soft signs of vascular injury determine immediate surgery vs. further workup. This decision point appears frequently and has zero tolerance for error.
When reviewing these common pitfalls, drill the decision points with surgery practice questions that focus specifically on management algorithms rather than memorization.
Integration with Other Step 2 CK Topics
Surgery doesnt exist in isolation on Step 2 CK. Integrate surgical knowledge with other clerkships:
Surgery + Internal Medicine:
Post-operative cardiac complications
DVT prophylaxis in surgical patients
Diabetic management perioperatively
Surgery + Emergency Medicine:
Trauma evaluation and stabilization
Acute abdomen differentials
Shock recognition and management
Surgery + Anesthesia:
Perioperative risk assessment
Post-operative pain management
Complications of general anesthesia
For comprehensive preparation, review internal medicine topics that commonly overlap with surgical scenarios.
High-Yield Mnemonics and Memory Aids
Beck Triad (Cardiac tamponade):
Elevated JVP
Hypotension
Muffled heart sounds
6 Ps of Acute Limb Ischemia:
Pain
Pallor
Pulselessness
Paresthesias
Paralysis
Poikilothermia (cold)
Glasgow Coma Scale:
Eyes: 4 = spontaneous, 3 = to voice, 2 = to pain, 1 = none
Verbal: 5 = oriented, 4 = confused, 3 = inappropriate, 2 = incomprehensible, 1 = none
Motor: 6 = obeys commands, 5 = localizes pain, 4 = withdraws, 3 = abnormal flexion, 2 = abnormal extension, 1 = none
These mnemonics become second nature when reinforced through spaced repetition flashcards that present the pattern in multiple clinical contexts.
Frequently Asked Questions
How much of USMLE Step 2 CK is surgery?
Surgery comprises approximately 15–20% of Step 2 CK, translating to 48-64 questions out of 318 total. This makes surgery the third-largest clinical topic after internal medicine and psychiatry. The percentage often surprises IMGs who may have limited surgical clerkship exposure.
What are the highest-yield surgery topics for Step 2 CK?
The highest-yield topics are trauma management (ATLS protocols), acute abdomen workups, post-operative complications, and vascular emergencies. These four areas account for roughly 75% of surgery questions. Focus on decision-making algorithms rather than operative techniques.
What surgical emergencies are on Step 2 CK?
Common surgical emergencies tested include cardiac tamponade, tension pneumothorax, ruptured AAA, acute limb ischemia, bowel obstruction with strangulation, and appendicitis with perforation. The exam focuses on immediate recognition and appropriate triage decisions.
How do I approach trauma questions on Step 2 CK?
Follow ATLS protocols systematically: primary survey (ABCDE), identify life-threatening injuries, assess patient stability, then choose between immediate surgery (unstable) or imaging first (stable). Most trauma questions test your ability to prioritize interventions correctly.
Is surgery harder than internal medicine on Step 2 CK?
Surgery questions are more binary and algorithm-driven than internal medicine, which can make them easier once you master the decision trees. However, surgery allows less room for error — missing a surgical emergency has severe consequences. The key is pattern recognition and systematic approaches.
What resources should I use to study surgery for Step 2 CK?
UWorld surgery questions are essential, supplemented by trauma and surgery-specific practice sets. Focus on resources that emphasize management decisions rather than operative techniques. Review actual ATLS protocols and acute care surgery guidelines for authoritative algorithms.
Final Strategy: The 4-Week Surgery Sprint
Week 1: Master trauma protocols and vascular emergencies Week 2: Acute abdomen workups and surgical indications Week 3: Post-operative complications and perioperative care Week 4: Integration and high-yield review
Surgery on Step 2 CK rewards systematic preparation. The exam tests clinical decision-making under pressure, not encyclopedic knowledge. Master the stability rule, practice trauma algorithms, and drill post-operative complication timelines. Your surgery score will follow.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.