How to Study Internal Medicine for USMLE Step 2 CK 2026: High-Yield Topics, Case Strategy and Exam Checklist
Master internal medicine for USMLE Step 2 CK with this comprehensive guide covering high-yield cardiology, nephrology, endocrinology topics, clinical vignette strategy, and exam day checklist for 2026.
How to Study Internal Medicine for USMLE Step 2 CK 2026: High-Yield Topics, Case Strategy and Exam Checklist
You are staring at your Step 2 CK prep schedule, and internal medicine takes up 40-50% of the entire exam. That means roughly 140 out of 280 questions will test your ability to think through clinical vignettes involving heart failure, diabetic ketoacidosis, acute kidney injury, and dozens of other high-stakes scenarios.
The math is brutal: master internal medicine or watch your score tank. But here's what most students get wrong — they treat IM like Step 1, memorizing pathways instead of learning clinical decision trees. Step 2 CK wants you to BE the doctor, not recite the textbook.
This guide breaks down the exact subtopics that show up most, the vignette patterns you'll see, and a study sequence that builds clinical reasoning instead of just facts. No fluff, no "comprehensive overviews" — just what works when you have limited time and need maximum points.
Why Internal Medicine Dominates Step 2 CK
Internal medicine isnt just the biggest section on Step 2 CK — it's the foundation that other specialties build on. When you see a surgery question about perioperative management, that's internal medicine. When pediatrics asks about adolescent diabetes, that's internal medicine. When psychiatry presents a patient with cardiac side effects from antipsychotics, that's internal medicine.
The exam tests 7 core IM subspecialties:
Cardiology (15-18% of total exam): heart failure, arrhythmias, acute coronary syndromes, valvular disease
Pulmonology (8-10%): asthma/COPD exacerbations, pneumonia, pleural effusions, pulmonary embolism
Nephrology (6-8%): acute kidney injury, chronic kidney disease, electrolyte disorders, acid-base
Gastroenterology (8-10%): GI bleeding, inflammatory bowel disease, liver disease, peptic ulcer disease
Endocrinology (6-8%): diabetes management, thyroid disorders, adrenal insufficiency
Hematology (5-7%): anemia workup, bleeding disorders, anticoagulation
Rheumatology (4-6%): lupus, rheumatoid arthritis, vasculitis, crystal arthropathies
Notice something? These percentages add up to more than 40%. That's because IM concepts bleed into every other section. The student who masters IM decision trees will recognize patterns across the entire exam.
The Step 2 CK Clinical Vignette Formula
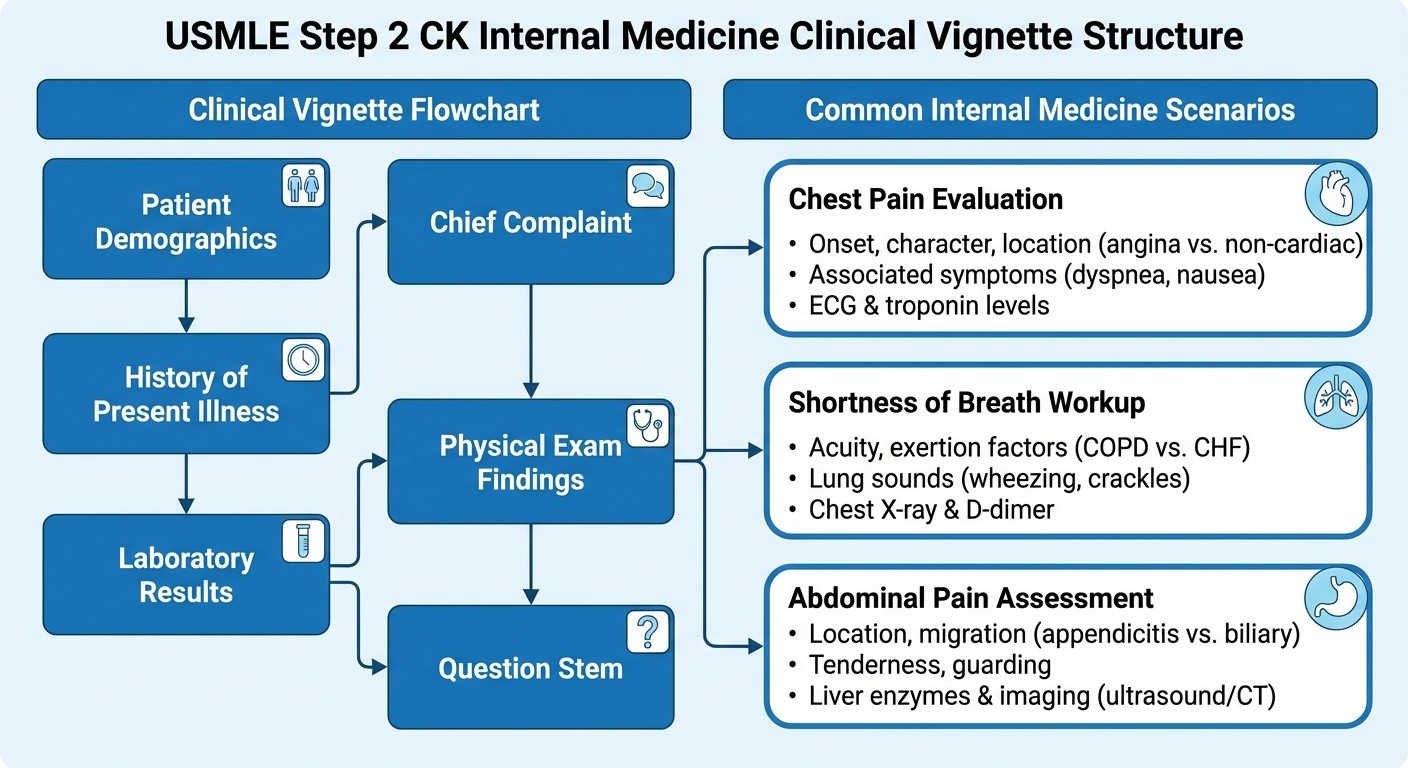
Every internal medicine question on Step 2 CK follows a predictable structure:
Setup: Patient demographics + chief complaint History: Timeline of symptoms + relevant positives/negatives Physical exam: Vital signs + focused findings Labs/imaging: Just enough data to make the diagnosis Question: What's the next best step, most likely diagnosis, or best treatment?
The key insight: Step 2 CK doesnt test rare diseases. It tests common diseases presenting in slightly unusual ways, or common presentations where students typically make specific mistakes.
For example, instead of a textbook MI presentation (crushing chest pain radiating to left arm), you'll see:
67-year-old diabetic woman with nausea, shortness of breath, and "indigestion" for 6 hours
Normal initial troponin, but ECG shows new T-wave inversions in leads II, III, aVF
Question asks: "What is the most appropriate next step?"
The trap: students who memorized "chest pain = MI" miss this. Students who learned "diabetic women present atypically, check serial troponins" nail it.
High-Yield Cardiology: Beyond the Obvious
Cardiology questions on Step 2 CK focus on acute management and risk stratification. You wont see basic anatomy or physiology — you'll see clinical decisions.
Most Tested Topics:
1. Acute coronary syndromes: STEMI vs NSTEMI vs unstable angina, timing of interventions 2. Heart failure: systolic vs diastolic, acute exacerbations, medication titration 3. Arrhythmias: atrial fibrillation management, wide-complex tachycardia approach 4. Valvular disease: when to operate, antibiotic prophylaxis 5. Hypertensive emergency: when to give IV meds, target blood pressures
The Pattern You'll See:
Instead of asking "What causes this murmur?", Step 2 CK asks:
"65-year-old with diabetes presents with crushing chest pain. ECG shows ST elevations in V1-V4. Troponin is 12.3. What is the most appropriate next step?" (Answer: emergent cardiac catheterization)
"Patient with known heart failure presents with shortness of breath. BNP is 2,400. Chest X-ray shows pulmonary edema. Current medications include lisinopril and metoprolol. What should be added?" (Answer: loop diuretic)
When studying cardiology, Oncourse's adaptive question bank automatically identifies if you're missing specific subtopics like acute MI management or heart failure pharmacology, then increases practice frequency in those exact areas until you demonstrate mastery.
Study Sequence:
1. Learn the acute coronary syndrome algorithm first — this shows up in 4-5 questions per exam
2. Master heart failure staging and medication classes
3. Focus on arrhythmia management algorithms (not just recognition)
4. Practice valvular disease decision trees
5. Review hypertension targets for different populations
Pulmonology: Think Clinical Context
Pulmonology questions test your ability to differentiate similar presentations and choose appropriate workup sequences.
Most Tested Topics:
1. Asthma vs COPD exacerbations: medication choices, criteria for discharge 2. Community-acquired pneumonia: severity scoring, antibiotic selection 3. Pulmonary embolism: risk stratification, anticoagulation decisions 4. Pleural effusions: when to tap, when to tube 5. Acute respiratory failure: invasive vs non-invasive ventilation
Common Vignette Patterns:
The COPD trap: Patient with known COPD presents with worsening shortness of breath. Chest X-ray shows hyperinflation. ABG shows CO2 retention. Question asks about oxygen delivery. (Answer: low-flow oxygen to avoid suppressing respiratory drive)
The pneumonia decision: Previously healthy 28-year-old with fever, cough, and left lower lobe consolidation. Question asks about antibiotic choice. (Answer: azithromycin for atypical coverage)
The AI explanations on every practice question help you understand why specific antibiotics are chosen for pneumonia or why certain oxygen delivery methods are preferred in COPD — the clinical reasoning that textbooks often skip.
High-Yield Facts:
PSI score >90 or CURB-65 ≥2 = hospitalize for pneumonia
Wells score >4 or PE likely = CT pulmonary angiogram
Exudative effusion: protein ratio >0.5, LDH ratio >0.6
COPD exacerbation: target O2 sat 88-92%, not 100%
Nephrology: Master the Algorithms
Nephrology questions focus on systematic approaches to acute kidney injury, electrolyte disorders, and acid-base problems.
Most Tested Topics:
1. Acute kidney injury: prerenal vs intrinsic vs postrenal workup 2. Chronic kidney disease: staging, complications, when to refer 3. Electrolyte disorders: hyponatremia, hyperkalemia management 4. Acid-base disorders: systematic interpretation approach 5. Glomerular disease: when to biopsy, treatment protocols
The AKI Decision Tree:
Step 2 CK loves AKI workup because it tests logical thinking:
1. Check urinalysis first
2. Calculate FeNa if prerenal suspected
3. Order renal ultrasound if postrenal possible
4. Consider nephrotoxic medications
5. Evaluate for systemic causes
Common Nephrology Traps:
Hyperkalemia: Students often jump to dialysis. Step 2 CK wants you to try medical management first (insulin/glucose, albuterol, sodium polystyrene)
Hyponatremia: Volume status determines treatment. Hypovolemic gets normal saline, euvolemic gets fluid restriction
CKD staging: Based on eGFR, not creatinine. Stage 4 CKD (eGFR 15-29) = nephrology referral time
When working through nephrology cases, spaced repetition helps solidify the drug dosing tables and GFR cutoffs that show up repeatedly — information that's easy to confuse under exam pressure.
Gastroenterology: Procedural Decisions Matter
GI questions emphasize when to scope, when to image, and how to manage bleeding emergencies.
Most Tested Topics:
1. GI bleeding: upper vs lower, when to scope urgently 2. Inflammatory bowel disease: UC vs Crohn's, flare management 3. Liver disease: hepatitis workup, cirrhosis complications 4. Peptic ulcer disease: H. pylori testing, medication management 5. Colorectal cancer screening: guidelines, follow-up intervals
GI Bleeding Algorithm:
Upper GI bleeding: Hematemesis, coffee-ground emesis, melena → upper endoscopy
Lower GI bleeding: Hematochezia in stable patient → colonoscopy (not urgent)
Massive bleeding: Unstable vitals → resuscitate first, then scope
High-Yield GI Facts:
H. pylori testing: stop PPIs 2 weeks before, antibiotics 4 weeks before
Colonoscopy screening: average risk at age 45, every 10 years
Hepatitis B surface antigen positive = active infection
Cirrhosis + ascites = check for spontaneous bacterial peritonitis
Endocrinology: Clinical Management Focus
Endocrine questions test acute management of diabetic emergencies and chronic disease monitoring.
Most Tested Topics:
1. Diabetes management: DKA vs HHS, insulin protocols 2. Thyroid disorders: hyperthyroid emergency, hypothyroid management 3. Adrenal disorders: adrenal insufficiency recognition, steroid dosing 4. Electrolyte disorders: diabetes insipidus vs SIADH 5. Reproductive endocrinology: PCOS, hypogonadism workup
Diabetes Emergency Patterns:
DKA: Anion gap acidosis + ketones + glucose >250. Treat with insulin + fluids
HHS: Glucose >600, osmolality >320, minimal ketones. Fluids first, then insulin
Hypoglycemia: Glucose <70. If conscious, give oral glucose. If unconscious, give glucagon or IV dextrose
Common Endocrine Traps:
Thyroid storm: Dont wait for lab results. Give methimazole + propranolol + steroids immediately
Adrenal insufficiency: Any patient on chronic steroids who becomes hypotensive needs stress-dose steroids
Diabetes screening: Fasting glucose ≥126, random ≥200, or HbA1c ≥6.5%
Hematology: Systematic Workups Win
Hematology questions focus on anemia evaluation and anticoagulation decisions.
Most Tested Topics:
1. Anemia workup: iron deficiency vs chronic disease vs megaloblastic 2. Bleeding disorders: von Willebrand vs hemophilia vs platelet disorders 3. Anticoagulation: warfarin vs DOACs, reversal agents 4. Thrombocytopenia: HIT vs ITP vs TTP recognition 5. Lymphadenopathy: when to biopsy, imaging choices
Anemia Algorithm:
1. Check MCV first (microcytic vs normocytic vs macrocytic)
2. Microcytic: iron studies (ferritin, TIBC, transferrin saturation)
3. Macrocytic: B12, folate, TSH, reticulocyte count
4. Normocytic: reticulocyte count, peripheral smear
Anticoagulation Decisions:
DVT/PE: DOAC preferred over warfarin for most patients
Atrial fibrillation: CHA2DS2-VASc score determines need
Mechanical valves: warfarin required, not DOACs
Major bleeding: stop anticoagulation, give reversal agent if needed
Rheumatology: Pattern Recognition
Rheumatology questions test classic presentations and appropriate workup sequences.
Most Tested Topics:
1. Systemic lupus erythematosus: ANA patterns, organ involvement 2. Rheumatoid arthritis: joint patterns, DMARD selection 3. Crystal arthropathies: gout vs pseudogout, acute management 4. Giant cell arteritis: when to treat empirically, biopsy timing 5. Vasculitis: ANCA patterns, organ involvement
Rheumatology Red Flags:
Giant cell arteritis: Age >50 + new headache + jaw claudication = start steroids immediately, dont wait for biopsy
Septic arthritis: Joint pain + fever = arthrocentesis before anything else
Lupus nephritis: Proteinuria + hematuria in lupus patient = renal biopsy
Study Strategy: Building Clinical Reasoning
The biggest mistake in Step 2 CK prep is studying each subspecialty in isolation. Internal medicine is about integration — seeing how cardiac, renal, and pulmonary systems interact in sick patients.
Phase 1: Foundation (Weeks 1-3)
Start with the Big 3: cardiology, pulmonology, nephrology. These appear most frequently and form the foundation for other topics.
Daily Structure:
Morning: Read high-yield review (UpToDate, Step Up to Medicine, or similar)
Afternoon: Practice 40-50 MCQs from your target subtopic
Evening: Review missed questions with focus on decision trees
Phase 2: Integration (Weeks 4-6)
Add gastroenterology, endocrinology, and hematology. Start mixing question sets — dont just do pure cardiology blocks.
Key Strategy: When reviewing a heart failure question, ask yourself: "What if this patient also had CKD? What if they had diabetes?" This builds the integration that Step 2 CK actually tests.
Phase 3: Pattern Recognition (Weeks 7-8)
Focus on rheumatology and complex cases. Practice identifying the "zebras" that show up as answer choices but arent the correct diagnosis.
Simulation Strategy: Do full-length practice exams that mix all subspecialties. Time yourself — Step 2 CK gives you 90 seconds per question, and IM vignettes are often longer than other specialties.
The adaptive question system tracks which IM subtopics you're struggling with and automatically adjusts your daily practice to include more nephrology AKI cases or heart failure management scenarios until you reach mastery level in each area.
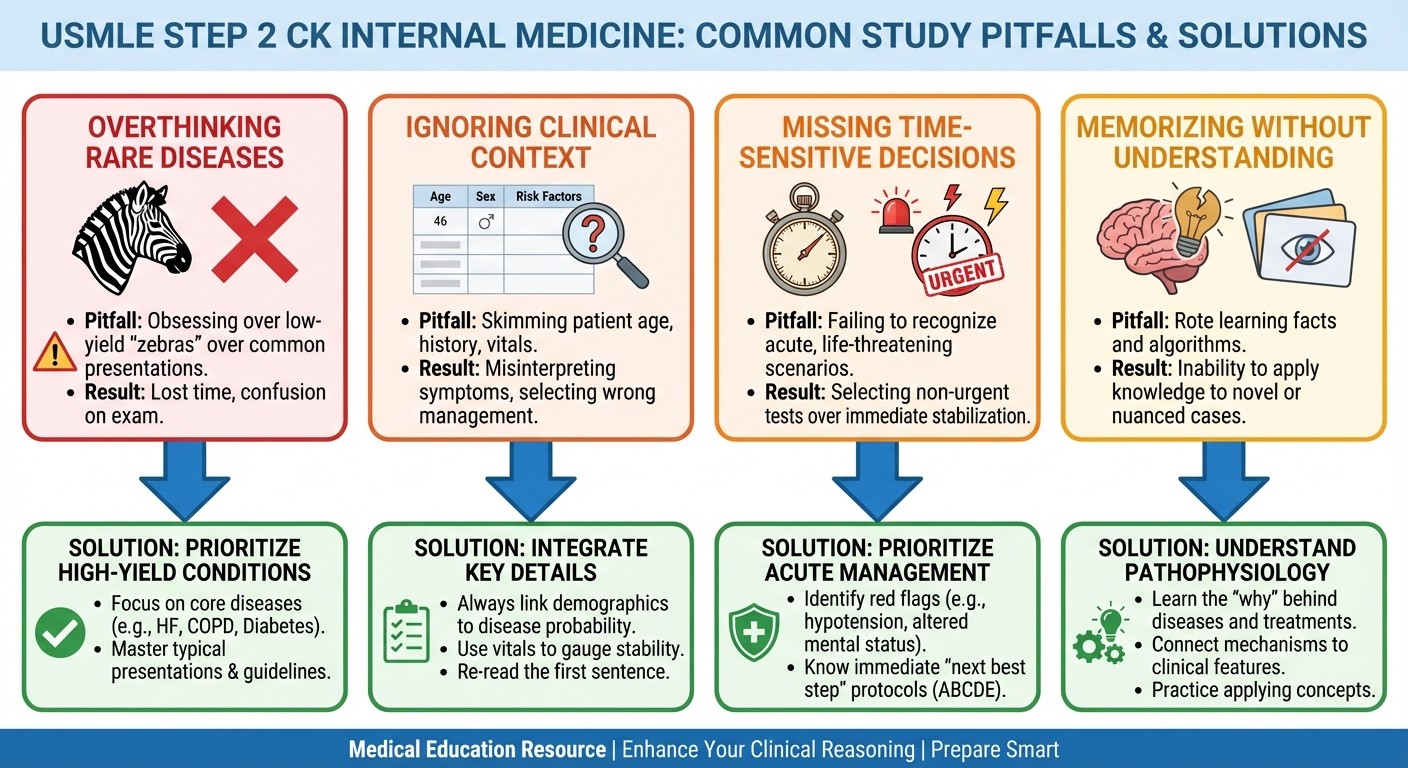
Common Pitfalls and How to Avoid Them
Pitfall #1: Overthinking Rare Diseases
Step 2 CK tests common diseases, not medical oddities. When you see a question about chest pain, think MI/PE/pneumonia before you consider pericarditis or Takotsubo cardiomyopathy.
Fix: Always consider the Big 3 differential for any chief complaint before moving to rare causes.
Pitfall #2: Ignoring Clinical Context
A 25-year-old marathon runner with chest pain gets a different workup than a 65-year-old diabetic smoker with the same complaint.
Fix: Patient age, comorbidities, and risk factors should guide your differential, not just the symptoms.
Pitfall #3: Missing Time-Sensitive Decisions
Step 2 CK often asks about "next best step" when time matters — like STEMI treatment or anaphylaxis management.
Fix: Learn the "cant wait" conditions: STEMI, DKA, sepsis, anaphylaxis, thyroid storm, adrenal crisis, hyperkalemia >6.5.
Pitfall #4: Memorizing Without Understanding
Knowing that lisinopril treats heart failure isnt enough. You need to know why ACE inhibitors improve mortality, when to hold them, and how to titrate doses.
Fix: For every medication, learn: mechanism, indication, contraindications, monitoring requirements, and side effects.
Exam Day Checklist: Internal Medicine Essentials
Pre-Test Mental Framework
Before starting each IM block, remind yourself:
1. Read the last line first (what is the question asking?)
2. Identify patient demographics and risk factors
3. Look for red flags that require immediate action
4. Think horses, not zebras (common diseases are common)
5. Choose the most conservative safe option when unsure
Must-Know Quick References
Vital Signs Red Flags:
SBP <90 or >220 = immediate intervention needed
HR >120 = look for sepsis, PE, bleeding, thyroid storm
O2 sat <90% = respiratory failure, consider intubation
Temp >38.5°C = infectious workup, blood cultures
Lab Value Red Flags:
K+ >6.0 = hyperkalemia protocol (insulin/glucose, albuterol)
Creatinine >3.0 = nephrology consult consideration
Troponin elevated = ACS protocol regardless of symptoms
Hemoglobin <7.0 = transfusion consideration
ECG Red Flags:
ST elevations = STEMI protocol (cath lab within 90 minutes)
Wide complex tachycardia = consider VT, treat with amiodarone
QTc >500 = torsades risk, check electrolytes, stop QT-prolonging drugs
Decision-Making Shortcuts
When stuck between two reasonable answers:
1. Safety first: Choose the option that wont harm the patient 2. Least invasive: Start with medical management before procedures 3. Most urgent: Address life-threatening conditions before chronic issues 4. Guidelines: Follow established protocols (ACLS, sepsis bundles, etc.)
High-Yield Drug Tables for Quick Review
Cardiology Medications
Condition | First-Line | Second-Line | Avoid |
|---|---|---|---|
Heart failure (systolic) | ACE inhibitor + beta-blocker | ARB, spironolactone | Verapamil, diltiazem |
Atrial fibrillation (rate) | Metoprolol, diltiazem | Digoxin | Beta-blockers in decompensated HF |
Hypertensive emergency | Nicardipine, clevidipine | Labetalol | Sublingual nitroglycerin |
STEMI | Aspirin + clopidogrel | Ticagrelor, prasugrel | Warfarin alone |
Pulmonology Medications
Condition | First-Line | Second-Line | Avoid |
|---|---|---|---|
COPD exacerbation | Albuterol + ipratropium | Prednisone | High-flow oxygen |
Asthma exacerbation | Albuterol | Magnesium sulfate | Beta-blockers |
Community-acquired pneumonia | Azithromycin | Levofloxacin | Doxycycline alone |
Pulmonary embolism | Rivaroxaban, apixaban | Warfarin | Aspirin alone |
Building long-term retention of these drug protocols requires spaced repetition at optimal intervals — reviewing heart failure medications every 3 days, then weekly, then monthly as your memory strengthens.
Sample Study Schedule: 8-Week Internal Medicine Focus
Weeks 1-2: Cardiology Foundation
Days 1-3: Acute coronary syndromes, ECG interpretation
Days 4-7: Heart failure classification, medication protocols
Days 8-10: Arrhythmia recognition and management
Days 11-14: Valvular disease, endocarditis, pericardial disease
Target: 50 cardiology MCQs daily, review all missed questions
Weeks 3-4: Pulmonology and Nephrology
Days 1-3: Asthma vs COPD, exacerbation management
Days 4-7: Pneumonia types, antibiotic selection, severity scoring
Days 8-10: AKI workup, electrolyte disorders
Days 11-14: CKD staging, acid-base interpretation
Target: Mixed cardio-pulm-nephrology blocks, 60 questions daily
Weeks 5-6: GI and Endocrinology
Days 1-4: GI bleeding algorithms, IBD management
Days 5-8: Liver disease, hepatitis workup
Days 9-12: DKA vs HHS, thyroid emergencies
Days 13-14: Adrenal disorders, diabetes management
Target: Integrated question blocks, all IM subspecialties
Weeks 7-8: Hematology, Rheumatology, and Integration
Days 1-3: Anemia workup, bleeding disorders
Days 4-6: Anticoagulation decisions, thrombosis
Days 7-10: Lupus, RA, crystal arthropathies
Days 11-14: Full-length practice exams, timed blocks
Target: Simulate real exam conditions, focus on time management
Frequently Asked Questions
How many internal medicine questions should I practice daily?
Start with 40-50 questions daily during foundation weeks, increase to 60-80 during integration phase. Quality matters more than quantity — spend 2-3 minutes reviewing each incorrect answer to understand the clinical reasoning.
Should I memorize normal lab values for Step 2 CK?
Yes, but focus on abnormal values that trigger immediate action. Know when creatinine indicates AKI, when troponin is significantly elevated, and when electrolyte levels require urgent correction. The exam provides reference ranges for most values.
How do I improve my timing on long internal medicine vignettes?
Read the question stem first to know what you're looking for, then read the vignette with purpose. Skip irrelevant details and focus on information that helps differentiate your top 2-3 diagnoses. Practice with timed blocks to build speed.
What's the most important internal medicine topic for Step 2 CK?
Cardiology, specifically acute coronary syndromes and heart failure management. These concepts appear in 15-20 questions per exam and form the foundation for understanding other cardiovascular topics across all specialties.
How do I handle questions where I dont know the diagnosis?
Use the ABC approach: Airway, Breathing, Circulation. Stabilize the patient first, then work through your differential. When unsure about diagnosis, choose the safest next step that wont harm the patient while gathering more information.
Should I focus on rare diseases or common presentations?
Focus on common diseases presenting in typical and atypical ways. Step 2 CK rarely tests true zebras — instead, it tests whether you can recognize heart failure in an elderly diabetic woman who presents with fatigue and ankle swelling rather than classic shortness of breath.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.