Back
USMLE Step 2 CK Pediatrics: High-Yield Topics, Key Presentations and Exam Strategy (2026)
Master USMLE Step 2 CK pediatrics with this comprehensive guide covering high-yield topics, classic presentations, developmental milestones, and strategic exam approach for 2026.
USMLE Step 2 CK Pediatrics: High-Yield Topics, Key Presentations and Exam Strategy (2026)
You stare at a pediatrics vignette. 8-month-old with fever, barking cough, stridor. Your mind races: croup vs epiglottitis vs foreign body. 60 seconds on the clock.
This is Step 2 CK pediatrics — where pattern recognition saves lives and scores points. Unlike Step 1's basic science focus, Step 2 CK tests your clinical reasoning with real patient presentations. In pediatrics, that means recognizing classic syndromes, knowing age-appropriate milestones, and choosing the right next step for a scared parent and sick child.
Pediatrics makes up 8-12% of Step 2 CK — roughly 25-30 questions out of 250. But these questions are high-yield: they test fundamental clinical skills you'll use regardless of specialty. Miss the signs of child abuse or botch a febrile seizure workup, and you'll regret it on test day.
This guide breaks down the most frequently tested pediatric topics, classic presentations that show up repeatedly, and the strategic approach that turns pediatrics from your weakness into your strength.
Most Tested Pediatric Topics on Step 2 CK
Developmental Milestones (High-Yield)
Expect 2-3 questions testing your knowledge of normal vs delayed development. The exam loves milestones at 2, 4, 6, 9, 12, 18, and 24 months.
Key ages and milestones:
2 months: Social smile, holds head up
4 months: Rolls front to back, laughs
6 months: Sits without support, transfers objects
9 months: Pulls to stand, pincer grasp
12 months: Walks independently, says "mama/dada" specifically
18 months: Walks up stairs, 20+ words, stacks 3 blocks
24 months: Runs, 2-word phrases, stacks 6 blocks
Red flags for developmental delay:
No social smile by 3 months
Not sitting by 9 months
Not walking by 18 months
No words by 16 months
Loss of previously acquired skills (regression)
When practicing developmental milestone questions, Oncourse's adaptive qbank automatically flags your weak areas — so if you keep missing 12-month milestones, you'll see more targeted practice until you nail the pattern.
Neonatology and Newborn Care
This section tests emergency recognition and routine newborn management. High-yield topics include:
Respiratory distress in newborns:
Respiratory Distress Syndrome (RDS): Premature infant, ground-glass appearance on CXR, requires surfactant
Transient Tachypnea of Newborn (TTN): Term infant, wet lung pattern, resolves in 24-48 hours
Meconium Aspiration: Post-term infant, thick meconium, pneumothorax risk
Neonatal jaundice patterns:
Physiologic jaundice: Appears day 2-3, peaks day 5-7
Pathologic jaundice: <24 hours old, rising >5 mg/dL/day, or >15 mg/dL total
Breast milk jaundice: Persistent beyond 2 weeks in breastfed infants
Congenital heart disease:
Critical presentations like hypoplastic left heart, tetralogy of Fallot, and transposition demand immediate recognition. Know which lesions are ductal-dependent and require PGE.
For neonatology practice, drill neonatology questions until you can spot cyanotic vs acyanotic heart disease in the first line of the vignette.
Infectious Diseases in Pediatrics
Pediatric ID questions focus on classic presentations and age-appropriate treatments.
Upper respiratory infections:
Croup: Barking cough, stridor, steeple sign on neck X-ray. Treatment: dexamethasone
Epiglottitis: Drooling, tripod position, thumbprint sign. Secure airway first
Bronchiolitis: <2 years old, wheezing, RSV season (fall/winter). Supportive care only
Fever without source:
0-28 days: Full sepsis workup, admit for empiric antibiotics
29-90 days: Depends on risk factors (Rochester criteria)
>90 days: Urine culture for girls <2 years, boys <6 months if uncircumcised
Classic pediatric infections:
Hand, foot, and mouth disease: Coxsackie virus, vesicles on palms/soles
Roseola: High fever 3-4 days, then diffuse rash as fever breaks
Kawasaki disease: 5+ days fever plus 4/5 criteria (rash, conjunctivitis, lymphadenopathy, extremity changes, oral changes)
The high-yield flashcards help cement these patterns — I found drilling Kawasaki criteria vs viral exanthem especially useful since both can present with fever and rash.
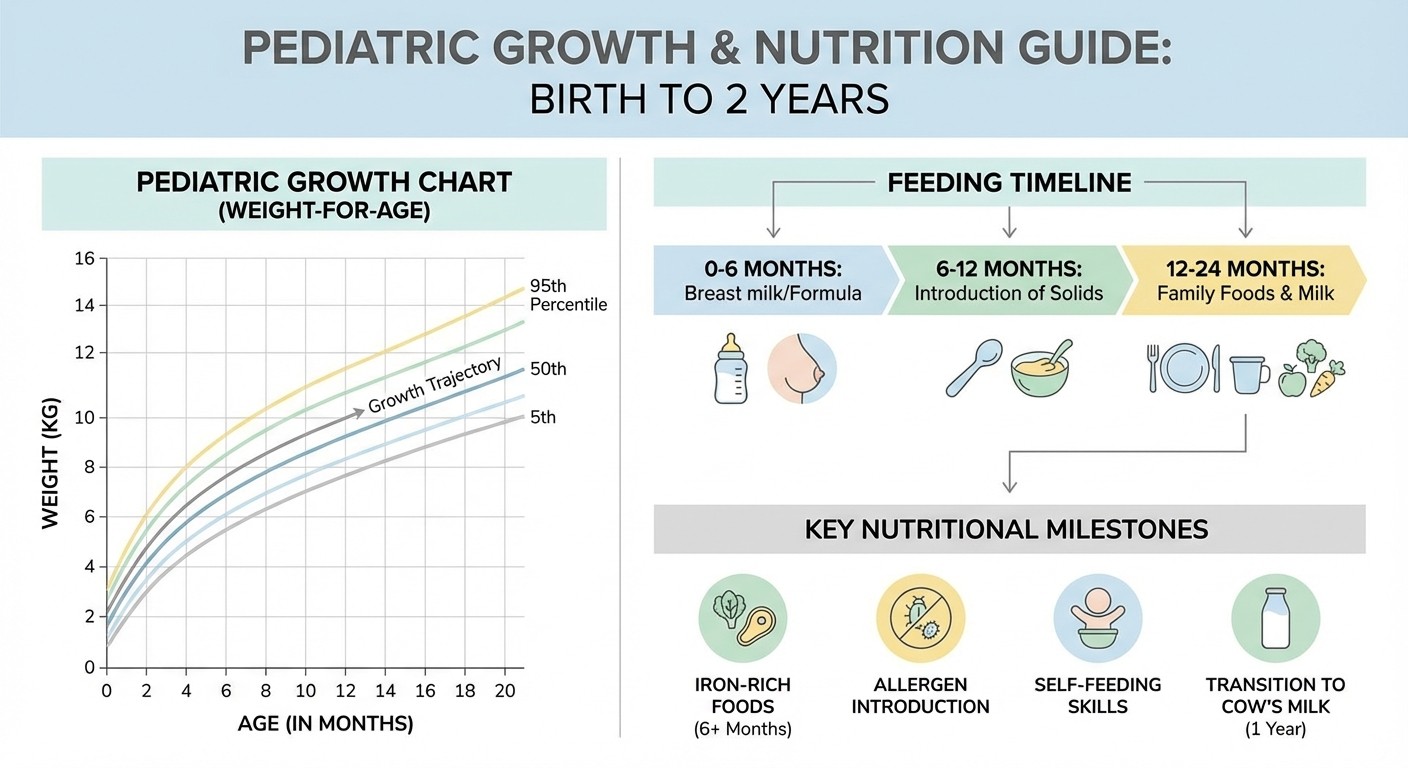
Growth and Nutrition
Step 2 CK tests practical nutrition counseling and growth chart interpretation.
Growth chart interpretation:
Plot height, weight, and head circumference
Crossing percentiles downward = concerning
Constitutional growth delay: Short stature but normal growth velocity
Failure to thrive: Weight <3rd percentile or crossing 2+ percentile lines
Feeding milestones:
4-6 months: Start solid foods
6 months: Iron-fortified cereals, pureed fruits/vegetables
9-12 months: Finger foods, self-feeding
12 months: Whole milk (not before!)
Iron deficiency anemia:
Most common nutritional deficiency in children. Risk factors include cow's milk before 12 months, excessive milk intake, and poor iron-rich food intake.
Adolescent Medicine
Often overlooked but consistently tested. Key areas include confidentiality, screening guidelines, and health maintenance.
Confidentiality rules:
Adolescents can consent for STI testing, contraception, and pregnancy care
Reportable conditions: child abuse, suicidal ideation, certain communicable diseases
HEADSS assessment: Home, Education, Activities, Drugs, Sexuality, Suicide
Screening recommendations:
Depression screening: Age 12+ annually
STI screening: Sexually active adolescents annually
HPV vaccine: Ages 11-12 (can start at 9)
Cervical cancer screening: Age 21 regardless of sexual activity onset
Child Abuse and Neglect
High-yield topic with significant legal implications.
Physical abuse red flags:
Injuries inconsistent with developmental stage
Multiple injuries in different healing stages
Specific patterns: loop marks, bite marks, immersion burns
Metaphyseal corner fractures in non-ambulatory children
Sexual abuse indicators:
Behavioral changes, age-inappropriate sexual knowledge
STIs in prepubertal children
Genital trauma (though most exams are normal)
Mandatory reporting:
All states require reporting suspected child abuse. You dont need "proof" — reasonable suspicion triggers the duty to report.
Classic Presentations You Must Know
Pediatric Emergencies
These presentations demand immediate recognition and action.
Febrile seizure:
6 months to 5 years old
Fever >38°C (100.4°F)
Simple: <15 minutes, generalized, no recurrence in 24 hours
Complex: >15 minutes, focal features, or recurrent
Workup: None needed for simple febrile seizures in 12-18 months old
Intussusception:
Peak age: 6-24 months
Colicky abdominal pain, vomiting, "currant jelly" stool
Sausage-shaped mass on palpation
Diagnosis: Ultrasound showing target sign
Treatment: Air enema (diagnostic and therapeutic)
Pyloric stenosis:
3-6 weeks old, more common in males
Projectile, non-bilious vomiting
Hypochloremic, hypokalemic metabolic alkalosis
Palpable olive-shaped mass
Diagnosis: Ultrasound showing thickened pylorus
Necrotizing enterocolitis:
Premature infants, especially <32 weeks
Feeding intolerance, abdominal distention, bloody stools
Pneumatosis intestinalis on abdominal X-ray
Treatment: NPO, antibiotics, surgery if perforation
Respiratory Presentations
Asthma exacerbation severity:
Mild: Peak flow >70% predicted, speaks in sentences
Moderate: Peak flow 40-69%, speaks in phrases
Severe: Peak flow <40%, speaks in words, accessory muscles
Life-threatening: Silent chest, cyanosis, altered mental status
Foreign body aspiration:
Sudden onset cough/choking while eating or playing
Unilateral wheezing or decreased breath sounds
Inspiratory stridor if upper airway, expiratory wheeze if lower
Diagnosis: Bronchoscopy (therapeutic too)
Strategic Approach to Pediatric Vignettes
Read for Age First
Age determines your differential diagnosis more than any other factor.
Neonates (0-28 days): Think sepsis, congenital anomalies, metabolic disorders Infants (1-12 months): RSV, intussusception, SIDS risk factors Toddlers (1-3 years): Accidental ingestions, febrile seizures, developmental concerns School age (4-11 years): ADHD, learning difficulties, sports injuries Adolescents (12-18 years): Risk-taking behaviors, depression, eating disorders
Vaccination Schedule Knowledge
Step 2 CK tests age-appropriate vaccines and catch-up schedules.
Core vaccines by age:
Birth: Hepatitis B
2 months: DTaP, IPV, Hib, PCV, Rotavirus
4 months: Same as 2 months
6 months: Same plus hepatitis B, influenza
12 months: MMR, Varicella, PCV, Hib
15 months: DTaP
4-6 years: DTaP, IPV, MMR, Varicella
Special situations:
Premature infants: Vaccinate by chronologic age, not corrected age
Immunocompromised: Avoid live vaccines (MMR, Varicella, Rotavirus)
Travel: Consider hepatitis A, typhoid, yellow fever
After working through Oncourse's pediatric question sets, the dashboard shows your accuracy across subspecialties — neonatology, infectious disease, development. This pinpoints exactly where to focus your remaining study time.
Developmental Red Flags vs Normal Variants
Know when to reassure parents vs when to refer for evaluation.
Normal variants:
Physiologic bowlegs until age 2
Flat feet until age 6
Breath-holding spells in toddlers
Stuttering in 2-4 year olds
Imaginary friends in preschoolers
Concerning findings requiring referral:
No words by 16 months
No 2-word phrases by 24 months
Loss of previously acquired skills
No social interaction or eye contact
Significant regression in any domain
Common Pediatric Step 2 CK Pitfalls
Age-Related Medication Errors
Aspirin: Never in children <18 years due to Reye's syndrome risk Honey: Not before 12 months (botulism risk) Fluoroquinolones: Generally avoided in children (cartilage effects) Tetracyclines: Not <8 years old (tooth discoloration)
Overordering Tests
Pediatric medicine emphasizes clinical diagnosis over extensive testing.
Dont order:
Urine culture for toilet-trained children without UTI symptoms
Chest X-ray for typical bronchiolitis
Blood work for simple febrile seizures
CT head for uncomplicated concussion
Do order:
Blood pressure in children >3 years old
Vision/hearing screening per schedule
Lead levels in high-risk children
Tuberculosis screening with high-risk factors
Missing Child Abuse
Step 2 CK will test your recognition of abuse patterns.
High-suspicion injuries:
Bucket-handle fractures (metaphyseal corner fractures)
Multiple fractures in different healing stages
Retinal hemorrhages in shaken baby syndrome
Bruises on protected areas (torso, ears, neck)
Remember: Your job isnt to prove abuse, but to recognize concerning patterns and report appropriately.
Practice Strategy for Pediatrics Success
Question Bank Approach
Focus on pattern recognition rather than memorizing facts.
For each pediatric vignette, ask:
1. What's the child's age and developmental stage?
2. What's the chief complaint and timeline?
3. What are the key physical findings?
4. What's the most likely diagnosis?
5. What's the next best step?
When using Oncourse's adaptive system for pediatrics practice, it automatically surfaces your weak areas — maybe you consistently miss neonatal jaundice questions but excel at developmental milestones. This targeted approach beats random question drilling.
Mnemonics for High-Yield Topics
Kawasaki disease criteria (need 4/5 plus fever >5 days):
CREAM: Conjunctivitis (bilateral), Rash, Extremity changes (edema/desquamation), Adenopathy (cervical >1.5cm), Mouth changes (strawberry tongue, cracked lips)
Cyanotic congenital heart diseases:
5 T's: Tetralogy of Fallot, Transposition of great arteries, Tricuspid atresia, Total anomalous pulmonary venous return, Truncus arteriosus
Signs of increased intracranial pressure:
HEADS UP: Headache, Eyes (papilledema), Altered mental status, Decreased consciousness, Seizures, Unequal pupils, Projectile vomiting
These mnemonics, along with others for pediatric emergency presentations, are built into Oncourse's flashcard system — each card links to question difficulty so you see the memory aid before attempting recall-based practice.
Time Management in Pediatric Questions
Pediatric vignettes often include worried parent quotes and family history details. Learn to extract key information quickly.
Read for these elements first:
1. Age and developmental context
2. Acute vs chronic presentation
3. Vital signs and key physical findings
4. Associated symptoms and timeline
Skip initially:
Detailed family social history
Extended review of systems
Non-contributory past medical history
You can always return to these details if needed for the specific question.
Frequently Asked Questions
How much pediatrics is on USMLE Step 2 CK?
Pediatrics comprises 8-12% of Step 2 CK questions, translating to roughly 25-30 questions out of 250 total. This makes it a significant but manageable portion that can impact your overall score.
Which pediatric topics are most frequently tested?
The highest-yield topics are developmental milestones, neonatology (especially respiratory distress and jaundice), pediatric infectious diseases (croup, bronchiolitis, classic viral exanthems), growth and nutrition disorders, and child abuse recognition. These areas consistently appear across multiple exam forms.
How should I approach developmental milestone questions?
Focus on key ages: 2, 4, 6, 9, 12, 18, and 24 months. Know the major gross motor, fine motor, language, and social milestones for each age. More importantly, memorize red flags for developmental delay — these often determine the correct answer in clinical scenarios.
What's the difference between croup and epiglottitis presentations?
Croup presents with barking cough, inspiratory stridor, and gradual onset in children 6 months to 6 years. Epiglottitis shows drooling, tripod positioning, high fever, and acute onset typically in children 2-7 years. On imaging, croup shows a steeple sign while epiglottitis shows a thumbprint sign.
How do I recognize child abuse on Step 2 CK?
Look for injuries inconsistent with the child's developmental stage, multiple injuries in different healing stages, specific patterns like loop marks or immersion burns, and metaphyseal corner fractures in non-ambulatory children. Behavioral indicators include fear of parents, age-inappropriate sexual knowledge, or regression in development.
Should I memorize the entire vaccination schedule?
Focus on key ages and vaccines: birth (Hepatitis B), 2/4/6 months (DTaP, IPV, Hib, PCV, Rotavirus), 12 months (MMR, Varicella), and 4-6 years boosters. Know that premature infants follow chronologic age for vaccines and immunocompromised children avoid live vaccines.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.