
Neonatology — MCQs

On this page
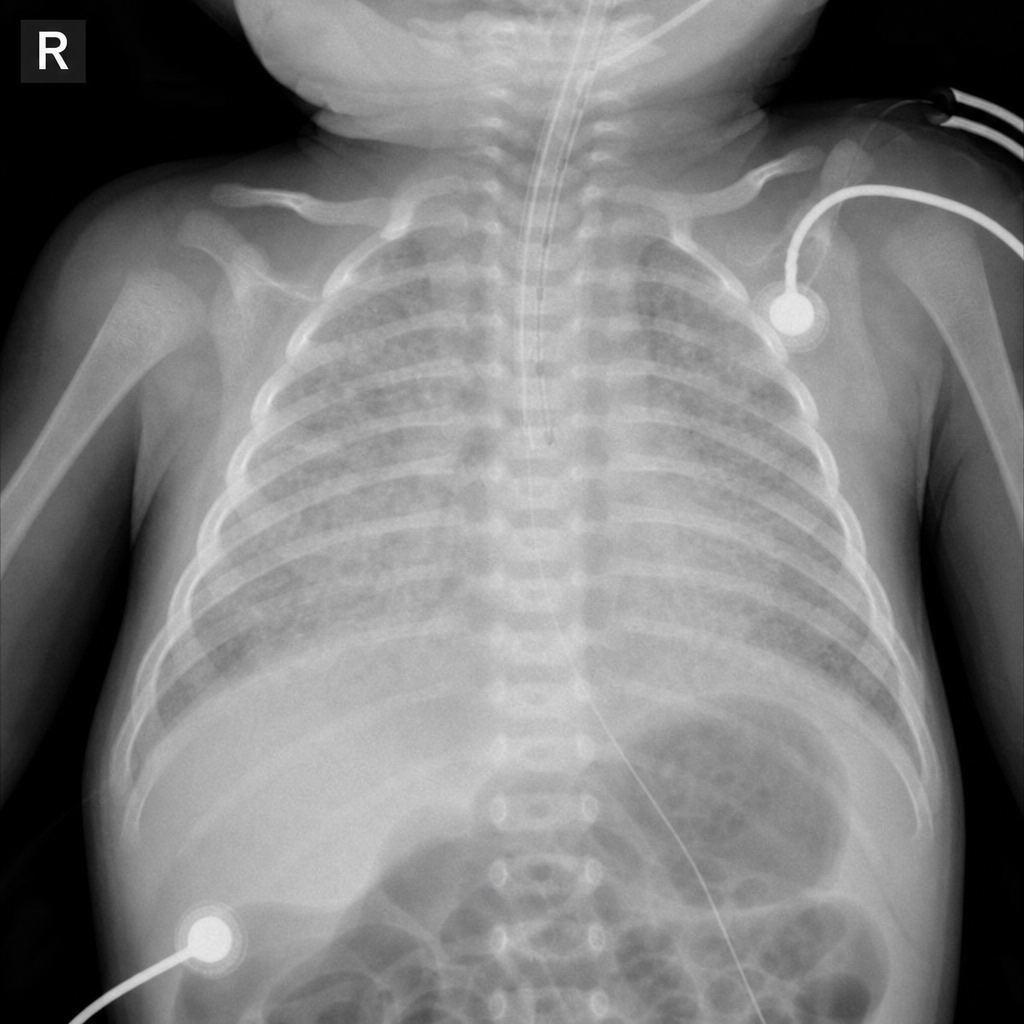
A preterm infant presents with respiratory distress soon after birth. The chest X -ray is given below. What is the most likely diagnosis?
A newborn has blue skin, heart rate less than 80/min, absent reflexes, and irregular respiration. What is the Apgar score?
A 3-hour-old newborn is found to have a blood glucose level of 38 mg/dL on routine screening. The neonate is asymptomatic. What is the most appropriate next step in management?
A pregnant woman with SLE delivers a neonate who is found to have a heart rate of 45 beats per minute. ECG confirms complete heart block. Which maternal antibody is most likely responsible?
A neonate presents with prolonged neonatal jaundice, an umbilical hernia, and generalized hypotonia. Which of the following is the most likely underlying diagnosis?
A 28-week preterm male neonate is delivered via emergency caesarean section due to placental abruption. Within minutes of birth, he develops grunting, subcostal retractions, and cyanosis with an SpO2 of 78% on room air. His Apgar scores are 4 and 6 at 1 and 5 minutes respectively. He is intubated and placed on mechanical ventilation. A chest X-ray is obtained (Image 1). Which of the following is the most appropriate immediate pharmacological intervention to address the underlying pathophysiology demonstrated on this X-ray?
What percentage of sucrose solution is used for newborn analgesia?
Which of the following is NOT a component of the APGAR score?
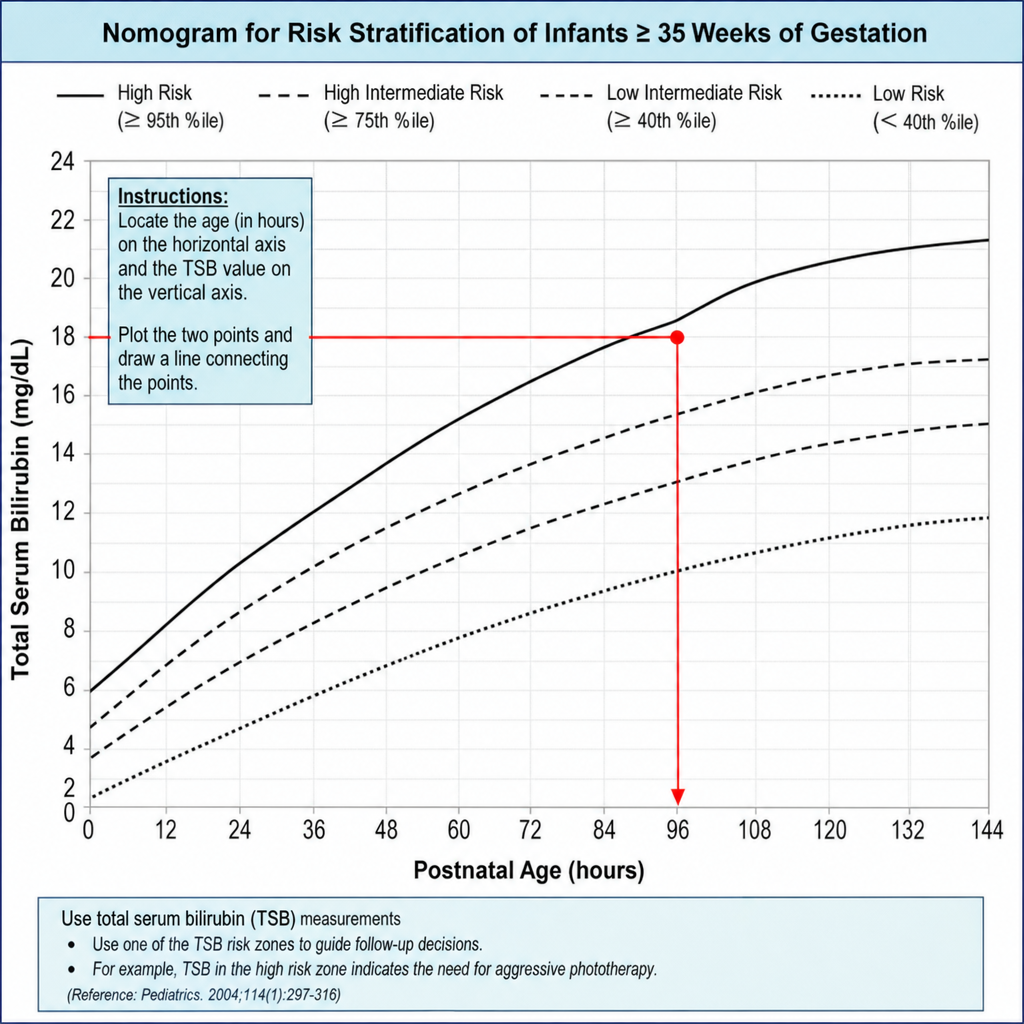
What is the probable bilirubin level of this neonate?
All of the following are true about congenital diaphragmatic hernia EXCEPT:
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app