How to Study Hematology & Oncology for USMLE Step 2 CK: High-Yield Topics, Clinical Patterns and Exam Strategy (2026)
Master USMLE Step 2 CK hematology oncology with high-yield anemia algorithms, coagulopathy charts, leukemia patterns, and oncologic emergency recognition strategies for 2026.
How to Study Hematology & Oncology for USMLE Step 2 CK: High-Yield Topics, Clinical Patterns and Exam Strategy (2026)
You are probably staring at a 47-question hematology block wondering why every vignette feels like a diagnostic puzzle with missing pieces. USMLE Step 2 CK treats Heme/Onc differently than Step 1 — instead of asking you to memorize cell cycle phases, it throws you into the clinical deep end with a 67-year-old presenting with fatigue and asks you to navigate the entire anemia workup.
Here's what most students get wrong: they study hematology and oncology as separate subjects. Bad move. Step 2 CK loves diagnostic overlap — the patient with "unexplained anemia" who actually has colon cancer, or the "pneumonia that won't resolve" that turns out to be leukemia with blast crisis.
This guide gives you the unified framework that actually works for test day. We'll cover the anemia algorithm that shows up in 60% of heme blocks, the coagulopathy chart that separates PT from PTT disorders, and the oncologic emergency patterns that can make or break your score.
Most importantly, we'll teach you to think like the exam thinks — not just what myelofibrosis looks like, but which clinical scenario makes you suspect it on a multiple-choice question.
How Heme/Onc Is Actually Tested on Step 2 CK
Step 2 CK doesnt test hematology knowledge — it tests diagnostic reasoning through hematologic presentations. Every question follows this pattern: clinical vignette → labs → "What is the most likely diagnosis?" or "What is the most appropriate next step?"
The exam loves these specific testing patterns:
The "Fatigue + Labs" Setup: 75% of anemia questions start with nonspecific fatigue, then give you a CBC with MCV and peripheral smear findings. Your job is recognizing the pattern, not memorizing every rare anemia type. The "Bleeding + Coag Panel" Scenario: PT/PTT results always appear together. Step 2 CK wants you to distinguish hemophilia A (isolated PTT elevation) from DIC (everything elevated) in under 90 seconds. The "Young Adult + Lymphadenopathy" Classic: Age matters enormously. Hodgkin lymphoma peaks at ages 20-30 and 55+. Non-Hodgkin lymphoma increases with age. The exam uses age as the first diagnostic clue. The "Oncologic Emergency" Trap: These questions disguise cancer complications as common medical problems. "Shortness of breath" might be superior vena cava syndrome. "Confusion + hypercalcemia" might be paraneoplastic syndrome from lung cancer.
Common distractors include listing multiple anemia types when only one fits the MCV pattern, or offering treatments before establishing the diagnosis. When practicing with USMLE hematology questions, focus on eliminating wrong answers by MCV and smear findings rather than trying to "know everything" about each condition.
Anemias: The High-Yield Diagnostic Algorithm
Step 2 CK anemia questions follow a predictable sequence: patient presentation → CBC with MCV → peripheral smear → diagnosis. Master this algorithm and you'll nail 80% of hematology questions.
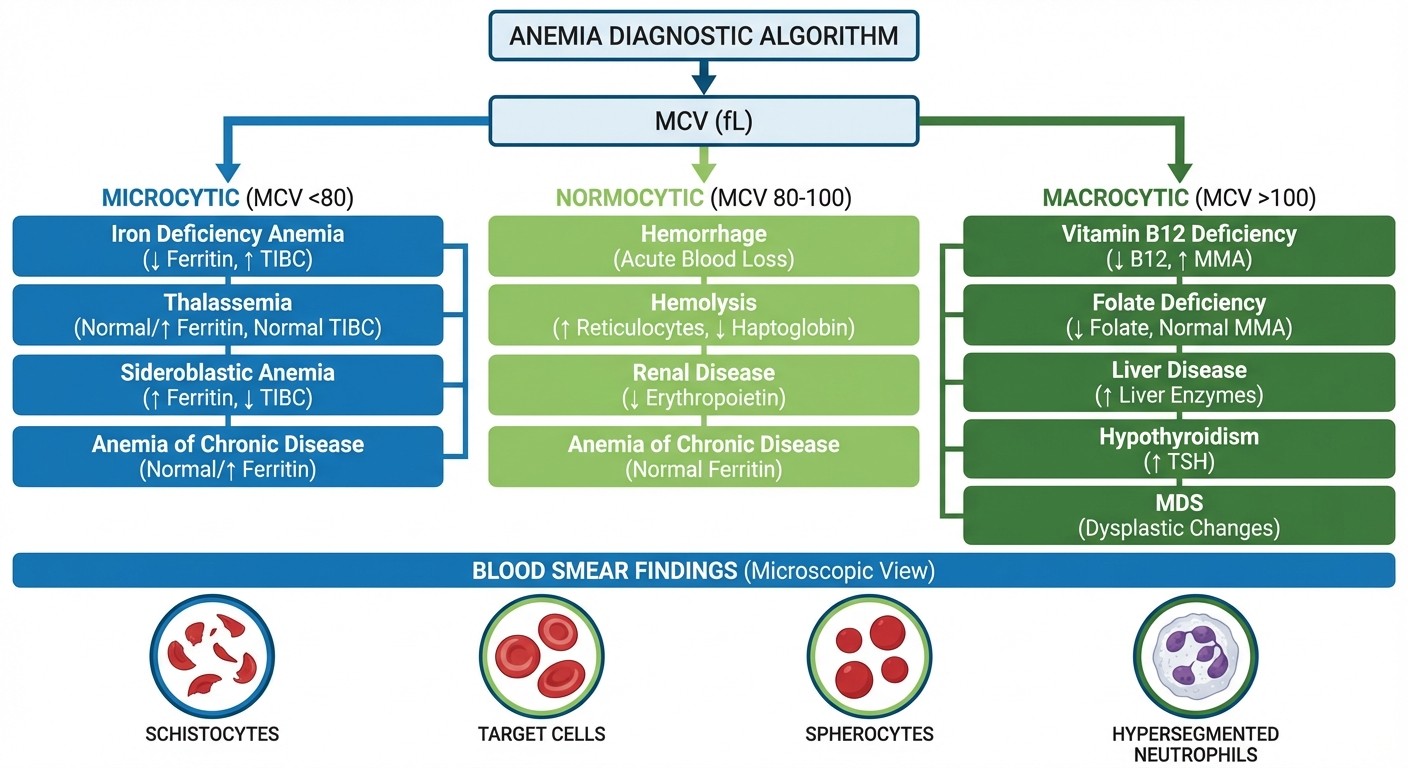
MCV-Based Initial Classification
Microcytic (MCV <80):
Iron deficiency (most common): Low ferritin, high TIBC, low transferrin saturation
Thalassemia: Normal/elevated ferritin, target cells on smear
Anemia of chronic disease (25% are microcytic): Elevated ferritin, low TIBC
Lead poisoning: Basophilic stippling on smear
Normocytic (MCV 80-100):
Anemia of chronic disease (75% are normocytic): Chronic illness history
Aplastic anemia: Pancytopenia, empty bone marrow
Acute blood loss: Recent trauma, GI bleeding, surgery
Chronic kidney disease: Low EPO levels
Macrocytic (MCV >100):
B12/folate deficiency: Hypersegmented neutrophils on smear
Alcoholism: Often with folate deficiency
Hypothyroidism: Check TSH
Medications: Methotrexate, hydroxyurea, antiretrovirals
Here's the Step 2 CK trick: when the vignette gives you a CBC, look at MCV first, then confirmatory tests. A 45-year-old woman with fatigue, MCV 72, and low ferritin gets diagnosed with iron deficiency — you dont need an extensive workup. But that same woman with MCV 72 and normal ferritin needs thalassemia studies.
The peripheral smear provides the diagnostic confirmation. Schistocytes suggest hemolytic anemia (think TTP, HUS, or DIC). Spherocytes point to hereditary spherocytosis or autoimmune hemolytic anemia. Target cells appear in thalassemia and liver disease.
Practice the iron deficiency anemia cases and anemia of chronic disease separately — Step 2 CK loves to test your ability to distinguish these two based on ferritin and TIBC levels.
Hemolytic Anemias: The "Schistocyte Story"
When you see schistocytes (fragmented RBCs) on a peripheral smear, think mechanical hemolysis. Step 2 CK tests three patterns:
TTP (Thrombotic Thrombocytopenic Purpura): Classic pentad includes thrombocytopenia, hemolytic anemia, neurologic symptoms, fever, and renal dysfunction. But most patients dont have all five — the exam typically gives you schistocytes + thrombocytopenia + altered mental status. HUS (Hemolytic Uremic Syndrome): More common in children, often follows E. coli O157:H7 diarrhea. The triad includes hemolytic anemia, thrombocytopenia, and acute renal failure. DIC (Disseminated Intravascular Coagulation): Secondary to sepsis, malignancy, or obstetric complications. Labs show elevated PT/PTT, low fibrinogen, elevated D-dimer, and schistocytes.
The discriminating feature: TTP has more neurologic symptoms, HUS has more renal involvement, and DIC has abnormal coagulation studies. For Clinical Rounds, working through these hemolytic emergency cases builds the pattern recognition you need — ordering the right sequence of labs (CBC, smear, coag studies, LDH) and selecting appropriate treatments based on the clinical presentation.
Coagulopathies: Decoding PT/PTT Results
Step 2 CK coagulopathy questions always provide PT/PTT results and ask you to identify the bleeding disorder. Memorize this chart — it shows up on every exam:
Condition | PT | PTT | Platelets | Key Features |
|---|---|---|---|---|
Hemophilia A | Normal | ↑ | Normal | Factor VIII deficiency, X-linked |
Hemophilia B | Normal | ↑ | Normal | Factor IX deficiency, X-linked |
Von Willebrand Disease | Normal | Normal/↑ | Normal/↓ | Most common inherited bleeding disorder |
Warfarin Effect | ↑ | Normal | Normal | Vitamin K antagonist |
Heparin Effect | Normal | ↑ | Normal | Antithrombin activation |
DIC | ↑ | ↑ | ↓ | Consumption of all factors |
Liver Disease | ↑ | ↑ | Normal/↓ | Synthetic dysfunction |
The Step 2 CK Approach: Start with PT and PTT results, then look at clinical context. A young male with hemarthrosis and isolated PTT elevation = hemophilia A until proven otherwise. Easy bleeding during dental procedures + normal PT/PTT + prolonged bleeding time = von Willebrand disease.
Von Willebrand disease deserves special attention because it's the most common inherited bleeding disorder but often has normal PT/PTT. The bleeding time (or PFA-100) is prolonged, and patients have mucocutaneous bleeding — nosebleeds, heavy menstrual periods, easy bruising.
DIC appears frequently on Step 2 CK because it complicates many conditions tested elsewhere: sepsis, obstetric emergencies, malignancy. The pathophysiology is consumption of platelets and clotting factors, leading to both bleeding and thrombosis. Labs show prolonged PT/PTT, low platelets, low fibrinogen, elevated D-dimer, and schistocytes on smear.
When reviewing hematology flashcards, focus on memorizing which tests are abnormal for each condition rather than the detailed pathophysiology.
Leukemias: Age Patterns and Diagnostic Clues
Step 2 CK leukemia questions use age as the primary diagnostic clue, followed by CBC findings and clinical presentation. Each leukemia has a characteristic age distribution and presentation pattern.
Acute Leukemias
AML (Acute Myeloid Leukemia):
Age: Primarily adults >60, but can occur at any age
CBC: Blasts >20%, often with pancytopenia
Smear: Auer rods (pathognomonic), myeloblasts
Complications: DIC (especially M3 variant), tumor lysis syndrome
ALL (Acute Lymphoblastic Leukemia):
Age: Peak at 2-5 years, second peak >50
CBC: Lymphoblasts, often with severe anemia/thrombocytopenia
Clinical: CNS involvement, mediastinal mass (T-cell variant)
Prognosis: Better in children than adults
Chronic Leukemias
CML (Chronic Myeloid Leukemia):
Age: 40-60 years
CBC: Extreme leukocytosis (often >100,000), left shift
Genetics: Philadelphia chromosome (BCR-ABL)
Clinical: Splenomegaly, later transforms to acute leukemia
CLL (Chronic Lymphocytic Leukemia):
Age: >65 years, most common leukemia in adults
CBC: Lymphocytosis, smudge cells on smear
Clinical: Lymphadenopathy, hypogammaglobulinemia
Complications: Richter transformation to aggressive lymphoma
The key Step 2 CK pattern: blast count determines acute vs chronic, cell type determines myeloid vs lymphoid, age and presentation narrow the diagnosis. A 25-year-old with mediastinal mass and lymphoblasts = T-cell ALL. A 70-year-old with smudge cells and lymphocytosis = CLL.
For rapid recall, the mnemonic AMLAUER helps remember AML features: Auer rods, Myeloblasts, Leukostasis, Adults, Uncontrolled bleeding, Emergent DIC, Requires immediate treatment. When working through Synapses puzzles, these mnemonics come up daily as active-recall challenges, building the instant pattern recognition Step 2 CK demands.
Lymphomas: Hodgkin vs Non-Hodgkin Differentiation
Step 2 CK lymphoma questions focus on distinguishing Hodgkin from Non-Hodgkin lymphoma, recognizing B symptoms, and identifying histologic clues. The key differences:
Hodgkin Lymphoma
Age: Bimodal distribution (20-30 and >55 years)
Spread: Contiguous lymph node involvement
B symptoms: Fever, night sweats, weight loss (present in 30%)
Histology: Reed-Sternberg cells (large cells with "owl-eye" nuclei)
Prognosis: Generally better than Non-Hodgkin
Non-Hodgkin Lymphoma
Age: Increases with age, median 60 years
Spread: Random, non-contiguous involvement
Subtypes: Many variants (DLBCL, follicular, mantle cell, etc.)
Clinical: More likely to involve extranodal sites
Prognosis: Variable depending on subtype
The Step 2 CK Pattern: Young adult with mediastinal mass and contiguous lymphadenopathy = Hodgkin until proven otherwise. Elderly patient with multiple non-contiguous lymph nodes and GI involvement = Non-Hodgkin lymphoma.
B symptoms are constitutional symptoms that indicate advanced disease: fever >38°C, drenching night sweats requiring clothing changes, and unintentional weight loss >10% over 6 months. Their presence affects staging and prognosis.
Reed-Sternberg cells are pathognomonic for Hodgkin lymphoma. These large cells have multiple nuclei or a bilobed nucleus with prominent nucleoli, giving an "owl-eye" appearance. Classic variants include lacunar cells and popcorn cells.
When studying lymphoma pathology, focus on the clinical presentation patterns rather than memorizing every subtype. Step 2 CK typically tests recognition of Hodgkin vs Non-Hodgkin rather than specific Non-Hodgkin variants.
Solid Tumor Oncology: Paraneoplastic Syndromes and Clinical Patterns
Step 2 CK approaches solid tumors through their clinical presentations and complications rather than staging details. Focus on these high-yield patterns:
Lung Cancer
Small Cell (SCLC):
Location: Central, hilar masses
Associations: Heavy smoking, paraneoplastic syndromes
Paraneoplastic: SIADH, Cushing syndrome, Lambert-Eaton syndrome
Prognosis: Aggressive, early metastasis
Non-Small Cell (NSCLC):
Types: Adenocarcinoma (peripheral), squamous cell (central)
Associations: Adenocarcinoma in nonsmokers increasing
Complications: Pancoast syndrome, SVC syndrome
Treatment: Surgical resection when possible
Colorectal Cancer
Risk factors: Age >50, IBD, family history, FAP, HNPCC
Screening: Colonoscopy starting age 45-50
Presentation: Change in bowel habits, iron deficiency anemia
Complications: Bowel obstruction, perforation, liver metastasis
Breast Cancer
Risk factors: BRCA mutations, family history, late menopause
Screening: Mammography 40-50 years (guidelines vary)
Types: Ductal carcinoma (invasive and in situ), lobular carcinoma
Receptor status: ER/PR positive, HER2 status affects treatment
Ovarian Cancer
Presentation: Often asymptomatic until advanced, abdominal distension
Tumor marker: CA-125 (elevated but not specific)
Histology: Serous cystadenocarcinoma most common
Prognosis: Poor due to late detection
The Step 2 CK focus is recognition of cancer presentations masquerading as other conditions. Iron deficiency anemia in a 55-year-old man = rule out colon cancer. Hypercalcemia + lung mass = paraneoplastic PTHrP from squamous cell lung cancer.
Oncologic Emergencies: Recognition and Initial Management
These emergencies appear frequently on Step 2 CK because they require immediate recognition and treatment. Master the clinical patterns:
Superior Vena Cava (SVC) Syndrome
Presentation: Facial swelling, shortness of breath, dilated chest wall veins Causes: Lung cancer (75%), lymphoma, thrombosis Diagnosis: CT chest with contrast Treatment: Radiation therapy, steroids, stenting
Tumor Lysis Syndrome
Presentation: Hyperkalemia, hyperphosphatemia, hypocalcemia, hyperuricemia Causes: High tumor burden cancers (leukemia, lymphoma) after chemotherapy Complications: Acute renal failure, cardiac arrhythmias Treatment: Aggressive hydration, allopurinol/rasburicase, dialysis
Neutropenic Fever
Definition: ANC <500 with fever >38°C Causes: Chemotherapy-induced neutropenia Approach: Blood cultures, empiric broad-spectrum antibiotics immediately Antibiotics: Cefepime, piperacillin-tazobactam, or meropenem
Hypercalcemia of Malignancy
Presentation: Confusion, polyuria, kidney stones, bone pain ("stones, bones, psychic moans") Causes: PTHrP (squamous cell cancers), osteolytic metastases, lymphomas Diagnosis: Elevated calcium with suppressed PTH, elevated PTHrP Treatment: IV fluids, loop diuretics, bisphosphonates
Spinal Cord Compression
Presentation: Back pain, weakness, sensory loss, bladder/bowel dysfunction Causes: Metastatic disease (breast, lung, prostate, kidney) Diagnosis: MRI spine immediately Treatment: High-dose steroids, radiation, surgical decompression
The Step 2 CK approach: these emergencies often present subtly in vignettes. A cancer patient with "confusion" might have hypercalcemia. "Shortness of breath" in a lung cancer patient could be SVC syndrome. Don't get distracted by the oncologic history — focus on the acute presentation.
When practicing emergency scenarios through Clinical Rounds, these cases build the rapid triage skills Step 2 CK demands — recognizing which symptoms require immediate intervention versus routine workup.
Test Day Strategy: Approaching Ambiguous Vignettes
Step 2 CK hematology/oncology questions can feel ambiguous because they mix clinical presentations with laboratory data. Here's your systematic approach:
Read the Question Stem First
Before reading the vignette, look at what they're asking: "Most likely diagnosis?" vs "Most appropriate next step?" vs "Best initial treatment?" This frames how you interpret the clinical data.
Use Age and Demographics
Age is often the biggest clue. Young adult with lymphadenopathy = consider Hodgkin. Elderly patient with anemia = think malignancy or chronic disease. Middle-aged person with bleeding = evaluate coagulopathy.
Follow the Lab Results Systematically
For Anemia: MCV first, then confirmatory tests (ferritin, B12, reticulocyte count) For Bleeding: PT/PTT pattern, then platelet count and clinical context For Cancer: Tumor markers and imaging results, then staging implications
Eliminate Obvious Wrong Answers
Many hematology questions include distractors that dont fit the lab pattern. If MCV is 65, eliminate all macrocytic causes. If PT/PTT are normal, eliminate coagulopathies that affect these values.
Recognize Common Step 2 CK Traps
Offering treatment before diagnosis is established
Choosing rare conditions when common ones fit better
Ignoring age-related disease probabilities
Mixing up hemophilia A vs B (both have isolated PTT elevation)
When You're Stuck Between Two Answers
Look for the discriminating clinical feature. TTP vs HUS both cause hemolytic anemia, but TTP has more neurologic symptoms. Iron deficiency vs thalassemia both cause microcytic anemia, but thalassemia has target cells on smear.
The key insight: Step 2 CK hematology/oncology questions test pattern recognition, not encyclopedic knowledge. Master the common presentations and diagnostic algorithms rather than memorizing every rare variant.
Remember that wrong answers on these complex questions unlock detailed explanations through Oncourse AI's Explanation Chat feature. Instead of spending 20 minutes searching through textbooks, you can ask specific questions like "What lab finding distinguishes TTP from HUS?" and get focused, Step 2 CK-specific answers that help you avoid similar mistakes.
Frequently Asked Questions
How many hematology/oncology questions appear on Step 2 CK?
Approximately 8-12% of Step 2 CK questions involve hematology/oncology, appearing across multiple blocks. Most integrate with other subjects — anemia workup in internal medicine cases, bleeding complications in surgery scenarios, or oncologic emergencies in emergency medicine settings.
Should I memorize all the cytogenetics for leukemias and lymphomas?
No. Step 2 CK focuses on clinical recognition rather than genetic details. Know the major ones: Philadelphia chromosome (BCR-ABL) for CML, t(15;17) for APL, and the association between Reed-Sternberg cells and Hodgkin lymphoma. Skip the detailed cytogenetics unless they directly impact clinical management.
How detailed should my knowledge of chemotherapy regimens be?
Very limited. Step 2 CK may ask about first-line treatments (like imatinib for CML or all-trans retinoic acid for APL), but it won't test specific drug combinations or dosing schedules. Focus on when to refer to oncology rather than memorizing treatment protocols.
What's the best way to differentiate iron deficiency from thalassemia?
Both cause microcytic anemia, but the pattern differs. Iron deficiency shows low ferritin, high TIBC, and low transferrin saturation. Thalassemia shows normal or elevated ferritin with target cells on peripheral smear. Family history often suggests thalassemia, while blood loss or dietary factors suggest iron deficiency.
How important are bone marrow biopsy findings for Step 2 CK?
Less important than clinical and basic lab findings. Know that aplastic anemia shows a hypocellular marrow, acute leukemias show >20% blasts, and chronic leukemias show different cell maturation patterns. The exam rarely tests detailed bone marrow morphology.
What's the most important thing to remember about oncologic emergencies?
Time sensitivity. SVC syndrome, spinal cord compression, tumor lysis syndrome, and neutropenic fever all require immediate recognition and treatment. The vignettes often bury these emergencies within longer clinical presentations — look for the key symptoms and act quickly.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.