
Hematology (anemias, clotting disorders) — MCQs

On this page
A 58-year-old woman with a 35-pack-year smoking history presents with progressive dyspnea on exertion over 6 months, a chronic productive cough, and two hospitalizations for respiratory infections in the past year. She uses an albuterol inhaler as needed. Her mMRC dyspnea score is 2 and CAT score is 18. Spirometry is performed. Post-bronchodilator FEV₁/FVC is 0.58 and FEV₁ is 48% of predicted. She has no wheezing at rest and her chest X-ray shows hyperinflation with flattened diaphragms. Which of the following changes to her maintenance regimen is most appropriate at this time?
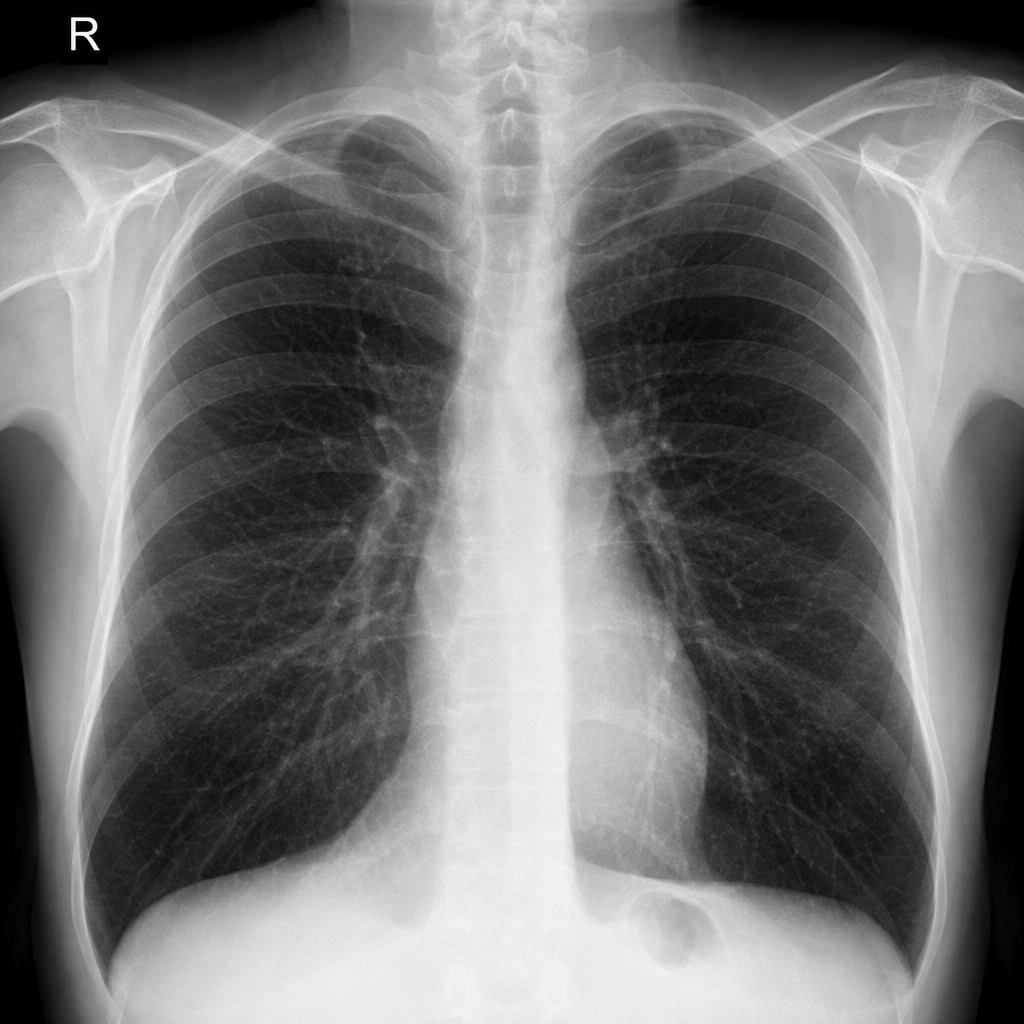
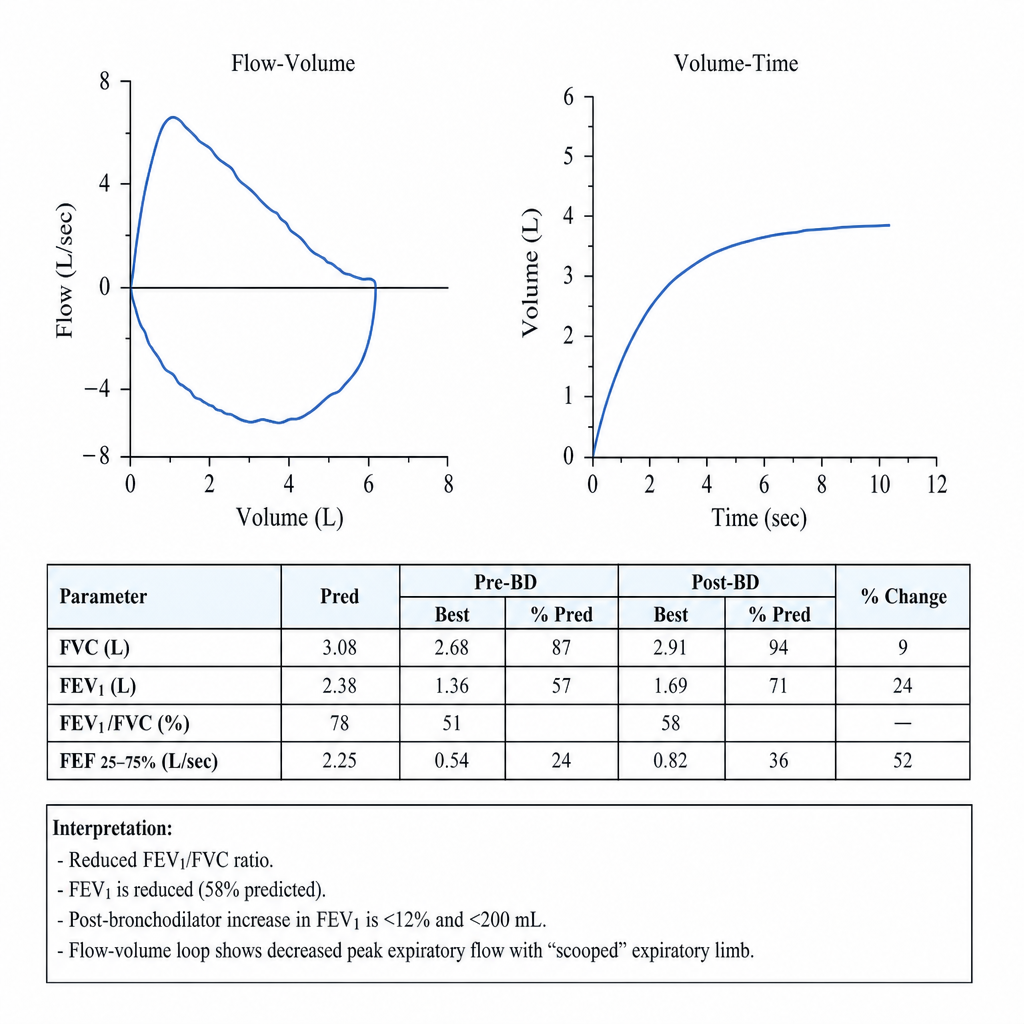
A 54-year-old woman with a 30-pack-year smoking history presents with 6 months of progressive exertional dyspnea and a chronic productive cough. She denies orthopnea or paroxysmal nocturnal dyspnea. Vitals are notable for oxygen saturation of 91% on room air. Chest auscultation reveals diffuse expiratory wheezes and a prolonged expiratory phase. Spirometry is performed; post-bronchodilator testing reveals an FEV1/FVC ratio of 0.62 with an FEV1 of 58% predicted, and repeat testing after bronchodilator administration shows less than 12% and less than 200 mL improvement in FEV1. Which of the following spirometric patterns is most consistent with this patient's presentation?
A 19-year-old college student returns from a mission trip to Kenya. Three weeks later, he develops fatigue, dark urine, and jaundice. Labs show: hemoglobin 8.1 g/dL (baseline 14 g/dL), MCV 92 fL, reticulocyte count 9%, total bilirubin 4.8 mg/dL (indirect), LDH 720 U/L. Peripheral smear shows bite cells and Heinz bodies. Malaria smears are negative. He reports taking primaquine for malaria prophylaxis. Which of the following is the most likely underlying condition?
A 35-year-old woman with lupus anticoagulant and history of two miscarriages is now 10 weeks pregnant. She had a DVT 3 years ago. She is currently asymptomatic. Her obstetrician requests recommendations for antithrombotic management throughout pregnancy and postpartum period. Synthesize the optimal comprehensive management strategy.
A 45-year-old woman presents with confusion and fever. Labs show: hemoglobin 7.8 g/dL, platelets 15,000/μL, creatinine 2.8 mg/dL, LDH 890 U/L, total bilirubin 3.1 mg/dL (indirect), undetectable haptoglobin. Peripheral smear shows numerous schistocytes. ADAMTS13 activity is 8% (normal >67%). She has no diarrheal illness. Coagulation studies (PT/aPTT) are normal. Evaluate the most appropriate immediate therapeutic intervention.
A 70-year-old man with metastatic pancreatic cancer on chemotherapy develops sudden dyspnea and hypoxia. CT pulmonary angiogram confirms bilateral pulmonary emboli. Platelet count is 45,000/μL (down from 180,000/μL two weeks ago). He has normal renal and liver function. Oncologist reports he has an estimated survival of 6-8 months. Evaluate the optimal long-term anticoagulation strategy.
A 24-year-old African American woman presents with severe bone pain and fever. She has sickle cell disease. Temperature is 39.2°C (102.6°F), blood pressure 110/65 mmHg. Hemoglobin is 6.1 g/dL (baseline 8.5 g/dL), reticulocyte count 0.5%, WBC 3,200/μL. Chest X-ray is clear. Blood cultures are pending. Analyze the clinical presentation and determine the priority intervention.
A 55-year-old man with chronic kidney disease (GFR 25 mL/min) develops deep vein thrombosis. He is started on low molecular weight heparin (LMWH) and warfarin. After 5 days, his INR is 2.8, but before stopping LMWH, laboratory studies show: platelet count decreased from 280,000/μL to 85,000/μL. He has no bleeding. Peripheral smear shows no schistocytes. Analyze the most likely diagnosis and appropriate action.
A 32-year-old woman presents with fatigue and dyspnea. Labs show hemoglobin 7.2 g/dL, MCV 68 fL, ferritin 8 ng/mL, and total iron binding capacity 450 μg/dL. She was started on oral ferrous sulfate 325 mg three times daily. After 4 weeks, her hemoglobin is unchanged at 7.3 g/dL. She reports taking the medication as prescribed. What factor most likely explains the lack of response?
A 65-year-old man with atrial fibrillation on warfarin (INR goal 2-3) presents to the emergency department after a fall with head trauma. His INR is 8.5. CT head shows a small subdural hematoma with no midline shift. He is alert and neurologically intact. Blood pressure is 145/85 mmHg. What is the most appropriate immediate management?
Practice by Chapter
Iron deficiency anemia
Practice Questions
Megaloblastic anemias
Practice Questions
Hemolytic anemias
Practice Questions
Anemia of chronic disease
Practice Questions
Sickle cell disease
Practice Questions
Thalassemias
Practice Questions
Platelet disorders
Practice Questions
Coagulation factor disorders
Practice Questions
Venous thromboembolism
Practice Questions
Hypercoagulable states
Practice Questions
Anticoagulation management
Practice Questions
Transfusion medicine
Practice Questions
Hematologic malignancies overview
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app