Back
USMLE Step 2 CK Gastroenterology and Hepatology: High-Yield Topics, Clinical Vignette Strategy and Exam Checklist (2026)
Master USMLE Step 2 CK gastroenterology and hepatology with high-yield topics, clinical vignette strategies, and exam checklist. IBD, GI bleeding, cirrhosis, hepatitis patterns for 2026.

USMLE Step 2 CK Gastroenterology and Hepatology: High-Yield Topics, Clinical Vignette Strategy and Exam Checklist (2026)
You're probably staring at a 400-page GI textbook wondering how you'll master hepatology AND gastroenterology before Step 2 CK. Here's the reality: Step 2 CK tests pattern recognition through clinical vignettes, not encyclopedic knowledge. The exam wants you to think like an intern making real decisions about real patients.
USMLE Step 2 CK gastroenterology questions make up roughly 8-10% of the exam — that's about 25-30 questions out of 318 total. But these aren't straightforward "which enzyme is elevated" questions. They're complex clinical scenarios where a 34-year-old presents with RUQ pain after fatty meals, or a 67-year-old has melena and a 6-month history of NSAID use.
The difference between a 240 and 260 in GI/hepatology isn't knowing more facts. It's recognizing patterns faster and avoiding common traps that trip up even strong students. This guide breaks down the exact high-yield topics, clinical reasoning frameworks, and vignette strategies you need to dominate GI questions in 2026.
Core High-Yield Gastroenterology Topics for Step 2 CK
Inflammatory Bowel Disease: Crohn's vs Ulcerative Colitis
Step 2 CK loves IBD because it tests both diagnostic thinking and management decisions. The classic vignette: 28-year-old with 3 months of bloody diarrhea, weight loss, and RLQ pain. Your job isn't just diagnosing IBD — it's distinguishing Crohn's from UC and knowing when to escalate care.
High-yield differentiating features:
Crohn's: Skip lesions, full-thickness inflammation, perianal disease, RLQ pain
UC: Continuous inflammation starting from rectum, bloody diarrhea predominant, left-sided pain
Clinical vignette red flags for Crohn's: Young patient with weight loss + perianal fistulas + RLQ mass + family history. The Oncourse adaptive qbank targets exactly these pattern recognition scenarios, adjusting difficulty based on whether you consistently miss Crohn's complications versus UC management. UC red flags: Bloody diarrhea + urgency + left-sided cramping + continuous mucosal involvement on colonoscopy.
The exam frequently tests when to use steroids (acute flares), when to start immunosuppressants (steroid-dependent), and complications like toxic megacolon or malignant transformation. Practice IBD clinical scenarios to nail the diagnostic approach.
GI Bleeding: Upper vs Lower, Acute Management
GI bleeding questions separate strong students from average ones because they test clinical decision-making under pressure. The exam scenarios range from obvious (hematemesis + coffee ground vomitus) to subtle (elderly patient on anticoagulation with unexplained anemia).
Upper GI bleeding approach:
1. Hemodynamic stability first — always
2. PPI therapy while preparing for endoscopy
3. Rockall score vs Glasgow-Blatchford for risk stratification
Classic upper GI bleeding vignette: 55-year-old with history of alcohol use presents with hematemesis and epigastric pain. Labs show Hgb 8.2, platelets 89k. The question tests your ability to recognize portal hypertension with likely esophageal varices. Lower GI bleeding patterns:
Diverticular: Painless, large volume, often right-sided in younger patients
Angiodysplasia: Elderly, chronic kidney disease, recurrent episodes
Ischemic colitis: Elderly with vascular disease, LLQ pain + bloody diarrhea
Performance analytics from question banks reveal students consistently miss the management of variceal bleeding — specifically when to use octreotide versus when endoscopic intervention is first-line. Review GI bleeding management protocols to solidify your approach.
Peptic Ulcer Disease and GERD
Step 2 CK tests PUD through management scenarios, not just H. pylori testing. The high-yield concept: when to test for H. pylori, how to test, and what to do with results.
H. pylori testing pearls:
Test if: Age <60 with dyspepsia, family history of gastric cancer, or recurrent PUD
Don't test if: Already on PPI (false negatives), recent antibiotics, or alarm features present
Urea breath test = gold standard for active infection
GERD management framework:
1. Lifestyle modifications first (weight loss, avoid triggers)
2. PPI trial for 4-8 weeks
3. If refractory: check compliance, consider H2 blocker combination
4. Red flags for endoscopy: dysphagia, weight loss, GI bleeding, age >50 with new symptoms
The classic trap: student sees "heartburn" and immediately jumps to PPI without considering red flags that mandate endoscopy first.
High-Yield Hepatology: Cirrhosis, Portal Hypertension, and Hepatitis
Cirrhosis Complications and Management
Hepatology questions on Step 2 CK focus heavily on recognizing and managing cirrhosis complications. The exam tests your ability to work through complex scenarios where multiple complications coexist.
Portal hypertension triad: Splenomegaly + thrombocytopenia + varices. When you see platelets <100k in a patient with known liver disease, think portal hypertension first. Ascites management strategy:
First-line: Sodium restriction + spironolactone
Refractory: Add furosemide, consider TIPS
Spontaneous bacterial peritonitis: PMN >250 = treat with ceftriaxone
Hepatic encephalopathy grades:
Grade 1: Mild confusion, altered sleep
Grade 2: Asterixis, disorientation
Grade 3: Stupor, marked confusion
Grade 4: Coma
The mnemonic "LIAR" helps remember precipitating factors: bleeding (Large volume), Infection, Alkalosis, Renal failure. AI explanations in adaptive question banks walk through the clinical reasoning behind recognizing these patterns rather than just memorizing lists.
Hepatitis Serologies: Decoding the Pattern
Step 2 CK loves hepatitis serology interpretation because it mimics real clinical decision-making. You'll see tables with multiple hepatitis markers and need to determine disease stage and infectivity.
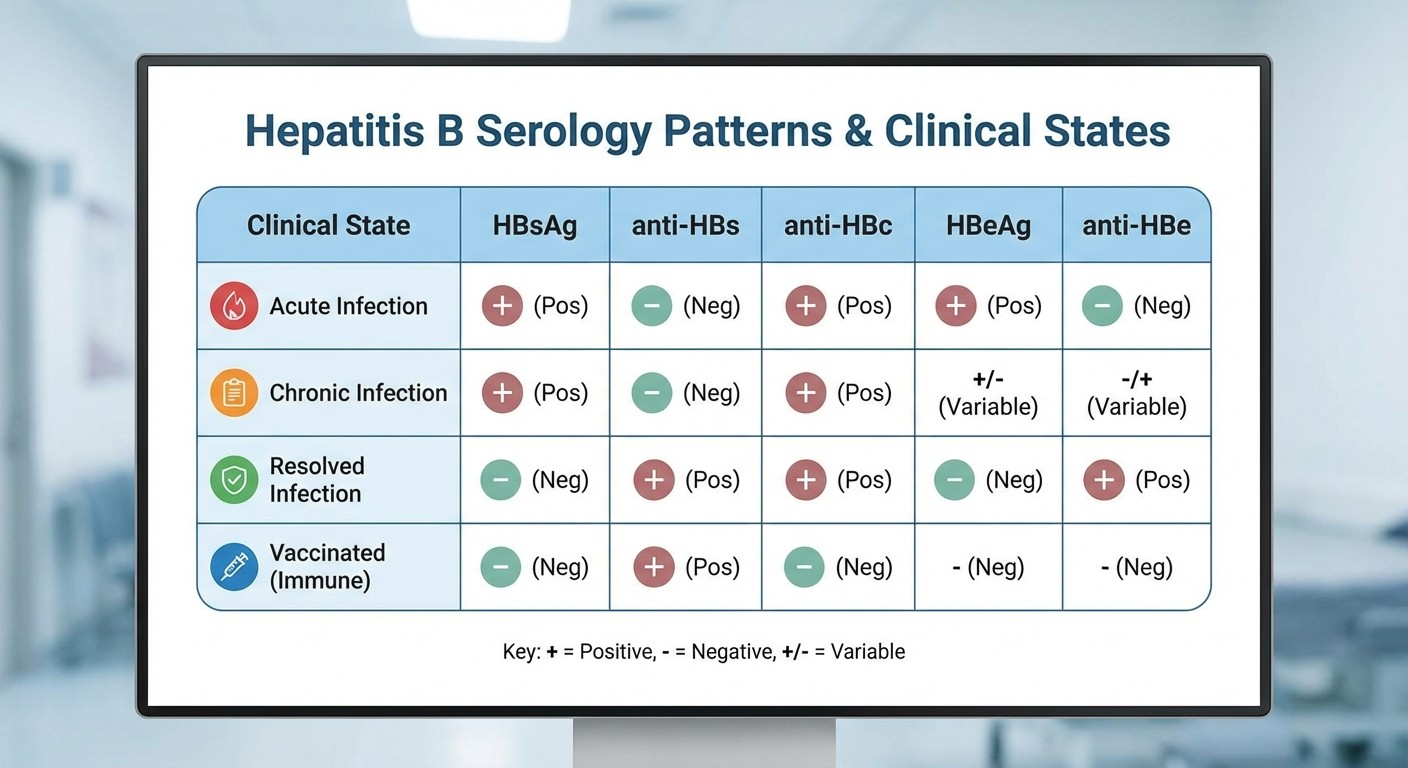
Key hepatitis B patterns:
Acute hepatitis B: HBsAg+, anti-HBc IgM+, HBeAg+
Chronic hepatitis B: HBsAg+ for >6 months, anti-HBc IgG+
Resolved infection: Anti-HBs+, anti-HBc+, HBsAg-
Vaccination: Anti-HBs+ only
Hepatitis C pearls:
Anti-HCV = exposure (doesn't distinguish active vs resolved)
HCV RNA = active infection
Cure rate with DAAs >95%
Acute Pancreatitis: Etiology and Complications
Pancreatitis questions test your ability to distinguish mild from severe disease and recognize complications early. The exam frequently presents scenarios where you need to decide between conservative management versus intervention.
Revised Atlanta Classification severity:
Mild: No organ failure, no complications
Moderate: Transient organ failure or complications without persistent organ failure
Severe: Persistent organ failure (>48 hours)
BISAP score factors: BUN >25, Impaired mental status, SIRS, Age >60, Pleural effusion. Score ≥3 predicts mortality.
When you see a question about acute pancreatitis with persistent pain after 48 hours + fever + leukocytosis, think complications. The classic trap: jumping to antibiotics before ruling out sterile necrosis with contrast CT.
Master pancreatitis management protocols through targeted practice questions that mirror real clinical scenarios.
Clinical Vignette Strategy: Pattern Recognition for Step 2 CK GI Questions
Recognizing GI Question Types
Step 2 CK GI vignettes follow predictable patterns. Learning to identify these patterns in the first 30 seconds saves time and improves accuracy.
Diagnostic vignette patterns:
"Young patient + chronic diarrhea + weight loss" = IBD workup
"Elderly + new dysphagia + weight loss" = esophageal malignancy until proven otherwise
"Alcoholic + ascites + spider angiomata" = cirrhosis complications
Management vignette patterns:
"Known diagnosis + new symptom" = test complication recognition
"Multiple treatment options listed" = test guidelines knowledge
"Patient with contraindications" = test alternative approaches
High-Yield Buzzwords and Clinical Pearls
Certain phrases in Step 2 CK vignettes point toward specific diagnoses. Recognizing these buzzwords instantly narrows your differential.
IBD buzzwords:
Crohn's: "Skip lesions," "full-thickness," "perianal fistulas," "cobblestoning"
UC: "Continuous inflammation," "crypt abscesses," "bloody diarrhea," "left-sided"
Liver disease buzzwords:
Alcoholic hepatitis: "AST:ALT ratio >2," "recent binge drinking," "tender hepatomegaly"
NASH: "Metabolic syndrome," "diabetes," "obesity," "elevated ALT"
Wilson's disease: "Young patient," "neuropsychiatric symptoms," "low ceruloplasmin"
GI bleeding buzzwords:
Variceal bleeding: "Known cirrhosis," "hematemesis," "thrombocytopenia"
Mallory-Weiss tear: "Forceful vomiting," "alcohol use," "chest pain"
Boerhaave syndrome: "Severe chest pain," "subcutaneous emphysema," "pneumomediastinum"
When studying with adaptive question banks, pay attention to these buzzword patterns. The system tracks whether you're missing questions due to poor pattern recognition versus knowledge gaps.
Common Distractors and How to Avoid Them
Step 2 CK question writers use predictable distractors that trap students who haven't developed clinical reasoning skills.
Classic GI distractors: 1. Ordering expensive tests unnecessarily: CT with contrast for uncomplicated GERD 2. Wrong sequence of management: Endoscopy before hemodynamic stabilization in GI bleeding 3. Missing contraindications: PPIs in patients on clopidogrel without considering interaction 4. Inappropriate antibiotic use: Treating asymptomatic H. pylori in elderly patients Hepatology distractors: 1. Overusing liver biopsy: When non-invasive markers sufficient for fibrosis staging 2. Missing drug interactions: Warfarin with alcohol in cirrhotic patients 3. Inappropriate ammonia levels: Ordering ammonia in obvious hepatic encephalopathy
The key strategy: always ask "What would I do as an intern?" rather than "What's the most complete workup possible?"
Decision-Making Frameworks for Complex GI Cases
The STOP-AND-THINK Method
For complex GI vignettes, use this systematic approach:
S - Stabilize (hemodynamics, airway, circulation) T - Think differential (most likely 3 diagnoses) O - Order appropriate tests (least invasive first) P - Plan initial management (evidence-based) AND T - Think complications (what could go wrong?) H - Have backup plan (if first-line fails) I - Include patient factors (age, comorbidities) N - Next steps (follow-up, monitoring) K - Know when to consult (surgery, GI, hepatology)
Approach to Undifferentiated Abdominal Pain
The Step 2 CK classic: "65-year-old with 6-hour history of severe abdominal pain." Your systematic approach determines whether you nail this question.
Immediate assessment priorities:
1. Hemodynamic stability
2. Pain character and location
3. Associated symptoms (nausea, vomiting, fever)
4. Physical exam findings (rebound, Murphy's sign, McBurney's point)
Red flags requiring immediate intervention:
Rebound tenderness + fever = peritonitis
Pulsatile abdominal mass = AAA
Biliary colic + jaundice + fever = Charcot's triad (ascending cholangitis)
Performance analytics from question platforms show students often miss the management sequence — they know the diagnosis but choose the wrong first step. Practice systematic approaches with immediate feedback on clinical reasoning.
When to Consult Surgery vs GI vs Hepatology
Step 2 CK tests your understanding of when primary care ends and specialty care begins. This knowledge separates students who think like interns from those stuck in preclinical mode.
Immediate surgical consult:
Perforated viscus (free air on imaging)
Massive GI bleeding (>4 units in 24 hours)
Toxic megacolon with IBD
Acute cholangitis not responding to antibiotics
GI consult indications:
Refractory GERD despite PPI therapy
Suspected IBD requiring colonoscopy
Variceal bleeding requiring endoscopy
Obscure GI bleeding needing capsule endoscopy
Hepatology consult indications:
Acute liver failure (INR >1.5 + encephalopathy)
Chronic liver disease evaluation for transplant
Complicated ascites requiring TIPS evaluation
Drug-induced liver injury with ALT >10x normal
Colorectal Cancer Screening and Polyp Management
Current Screening Guidelines for Step 2 CK
Colorectal cancer screening represents a high-yield topic because it combines preventive medicine with clinical decision-making. The 2026 guidelines emphasize shared decision-making and risk stratification.
Average risk screening (starting age 45):
Colonoscopy every 10 years
FIT testing annually
CT colonography every 5 years
Flexible sigmoidoscopy every 5 years + FIT every 3 years
High-risk populations requiring earlier/more frequent screening:
Family history of CRC in first-degree relative: Start age 40 or 10 years before relative's diagnosis
Personal history of IBD: Start 8-10 years after diagnosis, then annually
Known genetic syndromes: FAP (age 10-12), Lynch syndrome (age 20-25)
Polyp surveillance intervals:
1-2 small (<1cm) adenomas: 7-10 years
3-10 adenomas or >1cm adenoma: 3-5 years
>10 adenomas: 1-3 years (consider polyposis syndrome)
The exam frequently tests scenarios where patients have multiple risk factors. A 52-year-old with IBD and family history of CRC requires individualized screening, not standard guidelines.
Hereditary Cancer Syndromes
Step 2 CK loves testing genetic cancer syndromes because they require pattern recognition plus family counseling knowledge.
Lynch syndrome (HNPCC):
Autosomal dominant
MSI-high tumors
Associated cancers: colorectal, endometrial, ovarian
Screening: colonoscopy every 1-2 years starting age 20-25
Familial adenomatous polyposis (FAP):
APC gene mutation
>100 adenomatous polyps
Nearly 100% CRC risk without colectomy
Screening: flexible sigmoidoscopy annually starting age 10-12
Classic vignette: 24-year-old with family history of "multiple intestinal polyps" and early colon cancer. Key clue: multiple affected family members across generations.
Motility Disorders: GERD, Achalasia, and Gastroparesis
GERD: Beyond Acid Suppression
Step 2 CK tests GERD management complexity, not just PPI prescription. The exam scenarios often involve refractory symptoms or patients with contraindications to standard therapy.
Refractory GERD approach:
1. Optimize PPI timing (30-60 minutes before meals)
2. Rule out non-adherence and continued triggers
3. Consider pH monitoring to confirm acid-related symptoms
4. Evaluate for complications (Barrett's esophagus, stricture)
When to suspect complications:
Progressive dysphagia = stricture or malignancy
Iron deficiency anemia = chronic bleeding
Chronic cough = laryngeal reflux
Chest pain = cardiac vs esophageal spasm
The mnemonic "ALARM" helps remember red flags: Anemia, Loss of weight, Anorexia, Recent onset in age >50, Masses/Melena/dysphagia.
Achalasia: Primary vs Secondary
Achalasia questions test your ability to distinguish primary motility disorders from secondary causes and choose appropriate diagnostic studies.
Classic achalasia presentation:
Progressive dysphagia to solids AND liquids
Regurgitation of undigested food
Chest pain
Weight loss
Diagnostic approach:
1. Barium swallow: "bird's beak" appearance
2. Upper endoscopy: rule out pseudoachalasia (malignancy)
3. Manometry: confirmatory test showing absent peristalsis
Treatment options by subtype:
Type I (classic): Pneumatic dilation or laparoscopic Heller myotomy
Type II (with compression): Best response to treatment
Type III (spastic): Peroral endoscopic myotomy (POEM)
The exam trap: assuming all dysphagia in older patients is malignancy without considering motility disorders. AI explanations help you understand why certain age groups present with specific achalasia subtypes.
Step 2 CK GI/Hepatology Exam Checklist
Must-Know Conditions for Test Day
Use this checklist to ensure you've covered all high-yield topics with active recall and clinical application:
Inflammatory Conditions:
[ ] IBD: Crohn's vs UC diagnostic criteria and management
[ ] Peptic ulcer disease: H. pylori testing and eradication
[ ] Acute pancreatitis: severity scoring and complications
[ ] Cholecystitis: Murphy's sign and surgical indications
Liver Disease:
[ ] Cirrhosis complications: ascites, varices, hepatic encephalopathy
[ ] Hepatitis serologies: acute vs chronic vs resolved patterns
[ ] Drug-induced liver injury: acetaminophen vs other causes
[ ] Portal hypertension: TIPS indications and contraindications
GI Bleeding:
[ ] Upper GI bleeding: variceal vs non-variceal management
[ ] Lower GI bleeding: diverticular vs angiodysplasia vs IBD
[ ] Obscure GI bleeding: capsule endoscopy indications
[ ] Hemodynamic assessment and resuscitation priorities
Malignancy:
[ ] Colorectal cancer screening guidelines by risk category
[ ] Barrett's esophagus: surveillance intervals
[ ] Hepatocellular carcinoma: AFP and imaging surveillance
[ ] Pancreatic adenocarcinoma: CA 19-9 and staging
Motility/Functional:
[ ] GERD: PPI therapy and refractory management
[ ] Achalasia: manometry findings and treatment options
[ ] Gastroparesis: diabetic vs idiopathic causes
[ ] IBS: Rome criteria and functional vs organic differentiation
Quick Reference: Lab Value Interpretations
Liver function tests:
AST:ALT ratio >2: Alcoholic liver disease
ALT >AST: Viral hepatitis, drug-induced liver injury
Isolated alkaline phosphatase elevation: Biliary obstruction, bone disease
Low albumin + high PT/INR: Synthetic liver dysfunction
Pancreatic enzymes:
Lipase >3x normal: Acute pancreatitis (more specific than amylase)
Chronic elevation: Consider chronic pancreatitis or malignancy
Normal enzymes with clinical suspicion: Doesn't rule out pancreatitis
GI bleeding markers:
BUN:Creatinine ratio >20: Upper GI bleeding (blood protein absorption)
Haptoglobin low: Consider hemolysis vs massive bleeding
Lactate elevation: Ischemic bowel, severe bleeding with shock
Review comprehensive GI and hepatology content to reinforce these patterns through spaced repetition and active recall.
Frequently Asked Questions
What percentage of Step 2 CK questions cover gastroenterology and hepatology?
GI and hepatology typically represent 8-10% of Step 2 CK questions, translating to approximately 25-30 questions out of 318 total. These questions often integrate with other specialties (surgery for GI bleeding, emergency medicine for acute abdomen), making the actual clinical exposure higher.
How should I approach complex hepatitis serology tables on the exam?
Focus on the key markers: HBsAg (current infection), anti-HBs (immunity), and anti-HBc (exposure). Start with these three to determine if the patient has active infection, past infection, or vaccination-induced immunity. Then look at HBeAg and anti-HBe to assess infectivity in chronic cases.
When should I choose surgery consult versus GI consult in bleeding scenarios?
Choose surgery for: hemodynamic instability despite resuscitation, signs of perforation, or massive bleeding requiring >4 units. Choose GI for: stable patients needing endoscopic intervention, variceal bleeding management, or diagnostic endoscopy. The key is hemodynamic stability and immediacy of intervention needed.
What's the most reliable way to distinguish Crohn's disease from ulcerative colitis?
Focus on three key differentiators: anatomic distribution (skip lesions vs continuous), depth of involvement (transmural vs mucosal), and clinical presentation (perianal disease vs bloody diarrhea). If the vignette mentions perianal fistulas or RLQ mass, think Crohn's. If it emphasizes bloody diarrhea with tenesmus, think UC.
How do I approach refractory GERD questions on Step 2 CK?
Use the stepwise approach: first optimize PPI therapy (timing, dose, duration), then consider pH monitoring to confirm acid-related symptoms, rule out complications with endoscopy if red flags present, and finally consider surgical options (fundoplication) for medication-refractory disease with confirmed acid exposure.
Should I memorize all the Child-Pugh and MELD score components?
For Step 2 CK, understand the concepts rather than memorizing exact calculations. Know that both scores predict mortality in cirrhosis, MELD is used for transplant allocation, and higher scores indicate worse prognosis. Focus on recognizing when to calculate these scores (cirrhosis evaluation) rather than the arithmetic.
---
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.