Back
How to Study Dermatology for USMLE Step 2 CK 2026: High-Yield Topics, Classic Presentations and Exam Strategy
Master USMLE Step 2 CK dermatology with systematic approach to skin lesions, high-yield conditions, classic presentations, and evidence-based exam strategy for 2026.
How to Study Dermatology for USMLE Step 2 CK 2026: High-Yield Topics, Classic Presentations and Exam Strategy
You are staring at another dermatology vignette. The image shows some red, scaly patches on a patient's elbows. Is it psoriasis? Eczema? Contact dermatitis? You have 90 seconds to read the stem, analyze the image, and pick the right answer from five options that all sound plausible.
USMLE Step 2 CK dermatology questions trip up more students than they should. The exam includes 15-20 dermatology questions across your 8-hour test day. Miss half of these and you have lost 8-10 points that could have been easy wins. The problem isn't that dermatology is inherently difficult — it's that most students treat it like a visual memory game instead of learning the systematic approach that works.
This guide breaks down exactly how to master dermatology for Step 2 CK. You will learn the high-yield conditions that appear repeatedly, the classic presentations you must recognize instantly, and the systematic approach to tackle any skin lesion vignette. By the end, dermatology questions will become some of your most confident picks.
Why Dermatology Questions Feel Harder Than They Are
Step 2 CK dermatology questions test clinical reasoning, not just pattern recognition. The exam writers know that students memorize classic textbook images, so they present atypical cases, combine multiple conditions, or focus on management decisions rather than diagnosis.
Here's what makes these questions challenging:
Image Quality Variables: Pictures may show different lighting, skin tones, or stages of disease progression. A psoriasis plaque might look different on darker skin or during an acute flare versus chronic presentation. Clinical Context Matters: The same rash has different implications in a 25-year-old versus a 65-year-old. A scaly lesion on the face of an elderly patient raises melanoma concerns that wouldn't apply to a teenager with acne. Management Focus: Many questions skip straight to treatment. You need to know first-line therapies, when to refer to dermatology, and which conditions require immediate intervention versus watchful waiting. Associated Symptoms: Dermatology vignettes often include systemic symptoms. Joint pain with a rash suggests psoriatic arthritis. Fever with petechiae points to infectious or hematologic causes.
The key insight: treat dermatology like internal medicine with a visual component. Focus on pathophysiology, risk factors, and evidence-based management rather than just memorizing pictures.
High-Yield Dermatology Conditions for Step 2 CK
Inflammatory Skin Diseases
Psoriasis appears in 2-3 questions per exam. Look for well-demarcated, red plaques with silvery scale on extensor surfaces (elbows, knees, scalp). Key buzzwords: Koebner phenomenon (lesions at sites of trauma), nail pitting, arthritis symptoms. First-line treatment: topical corticosteroids and vitamin D analogs. Oncourse AI adaptive question bank includes multiple psoriasis vignettes that test both classic and atypical presentations — practice recognizing guttate psoriasis in young patients after strep throat. Atopic Dermatitis/Eczema shows up as chronic, pruritic lesions in flexural areas (antecubital and popliteal fossae). Often starts in childhood with personal or family history of asthma or allergies. Treatment ladder: moisturizers → topical steroids → topical calcineurin inhibitors → systemic therapy for severe cases. Contact Dermatitis presents as acute vesicular eruption in areas of contact with allergens or irritants. Common triggers include poison ivy (linear pattern), nickel (jewelry), or occupational exposures. Management: identify and avoid trigger, topical steroids for symptomatic relief.
Infectious Skin Conditions
Cellulitis appears frequently as painful, red, warm, swollen skin with ill-defined borders. Key distinction from abscess: cellulitis lacks fluctuance and central necrosis. First-line oral treatment: cephalexin for mild cases. IV clindamycin or vancomycin for severe infections or MRSA risk factors. Impetigo shows honey-crusted lesions, typically in children. Two types: non-bullous (more common, caused by Staph aureus or Strep pyogenes) and bullous (Staph aureus with toxin production). Treatment: topical mupirocin for limited lesions, oral antibiotics for extensive disease. Herpes Simplex presents as grouped vesicles on an erythematous base. HSV-1 typically affects the face (cold sores), HSV-2 affects genital areas. Recurrent episodes are shorter and less severe. Treatment: oral acyclovir, valacyclovir, or famciclovir. Varicella Zoster has two presentations. Primary infection (chickenpox) shows generalized vesicular rash in different stages. Reactivation (shingles) presents as painful vesicles in a dermatomal distribution. Post-herpetic neuralgia is the most common complication in elderly patients.
Neoplastic Skin Diseases
Basal Cell Carcinoma is the most common skin cancer but rarely metastasizes. Look for pearly, rolled borders with central ulceration or telangiectasias. Most common on sun-exposed areas. Treatment: excision, Mohs surgery for high-risk locations. Squamous Cell Carcinoma has higher metastatic potential than BCC. Appears as scaly, hyperkeratotic papules or nodules. Risk factors include chronic UV exposure, immunosuppression, and chronic wounds. Treatment: excision with adequate margins. Melanoma is the deadliest skin cancer. Use ABCDE criteria: Asymmetry, Border irregularity, Color variation, Diameter >6mm, Evolving characteristics. Any suspicious lesion requires urgent dermatology referral and biopsy. Treatment depends on staging but includes wide local excision ± sentinel lymph node biopsy. Actinic Keratosis represents pre-malignant lesions with 10-15% risk of progression to SCC. Appears as rough, scaly papules on sun-exposed skin. Treatment options include cryotherapy, topical 5-fluorouracil, or imiquimod.
Autoimmune Blistering Diseases
Pemphigus Vulgaris causes intraepidermal blisters that rupture easily (positive Nikolsky sign). Often starts in oral mucosa before skin involvement. Diagnosis confirmed by skin biopsy showing acantholysis and positive anti-desmoglein antibodies. Treatment: systemic corticosteroids ± immunosuppressants. Bullous Pemphigoid produces subepidermal, tense blisters that don't rupture easily (negative Nikolsky sign). Typically affects elderly patients with pruritic urticarial plaques that progress to blisters. Treatment: topical or systemic corticosteroids depending on extent.
Classic Visual Presentations You Must Know
Understanding morphology helps you decode any skin lesion vignette. Here are the patterns that appear repeatedly:
Papulosquamous Patterns: Raised lesions with scale. Think psoriasis (thick, silvery scale), seborrheic dermatitis (greasy, yellow scale), or pityriasis rosea (Christmas tree pattern on back). Vesiculobullous Patterns: Fluid-filled lesions. Small vesicles suggest herpes simplex or contact dermatitis. Large, tense bullae point to bullous pemphigoid. Easily ruptured blisters suggest pemphigus. Purpuric Patterns: Non-blanching red/purple lesions. Petechiae (<3mm) suggest platelet problems. Purpura (3-10mm) may indicate vasculitis or coagulopathy. Ecchymoses (>10mm) suggest trauma or bleeding disorders. Annular Patterns: Ring-shaped lesions. Tinea corporis shows central clearing with active border. Granuloma annulare has smooth, flesh-colored papules in rings. Erythema migrans (Lyme disease) expands outward from tick bite.
When reviewing image-based questions, Oncourse smart flashcard system surfaces key morphology descriptors at optimal intervals — build your dedicated derm deck sorting lesions by primary morphology, then layer in specific diagnoses.
Systematic Approach to Dermatology Vignettes
Don't just stare at the picture and guess. Use this structured approach for every skin lesion question:
Step 1: Read the Clinical Context First
Before looking at the image, extract key information from the vignette:
Patient age and demographics
Location of lesions
Duration and progression
Associated symptoms (itch, pain, fever)
Relevant medical history
Current medications
Step 2: Analyze Image Systematically
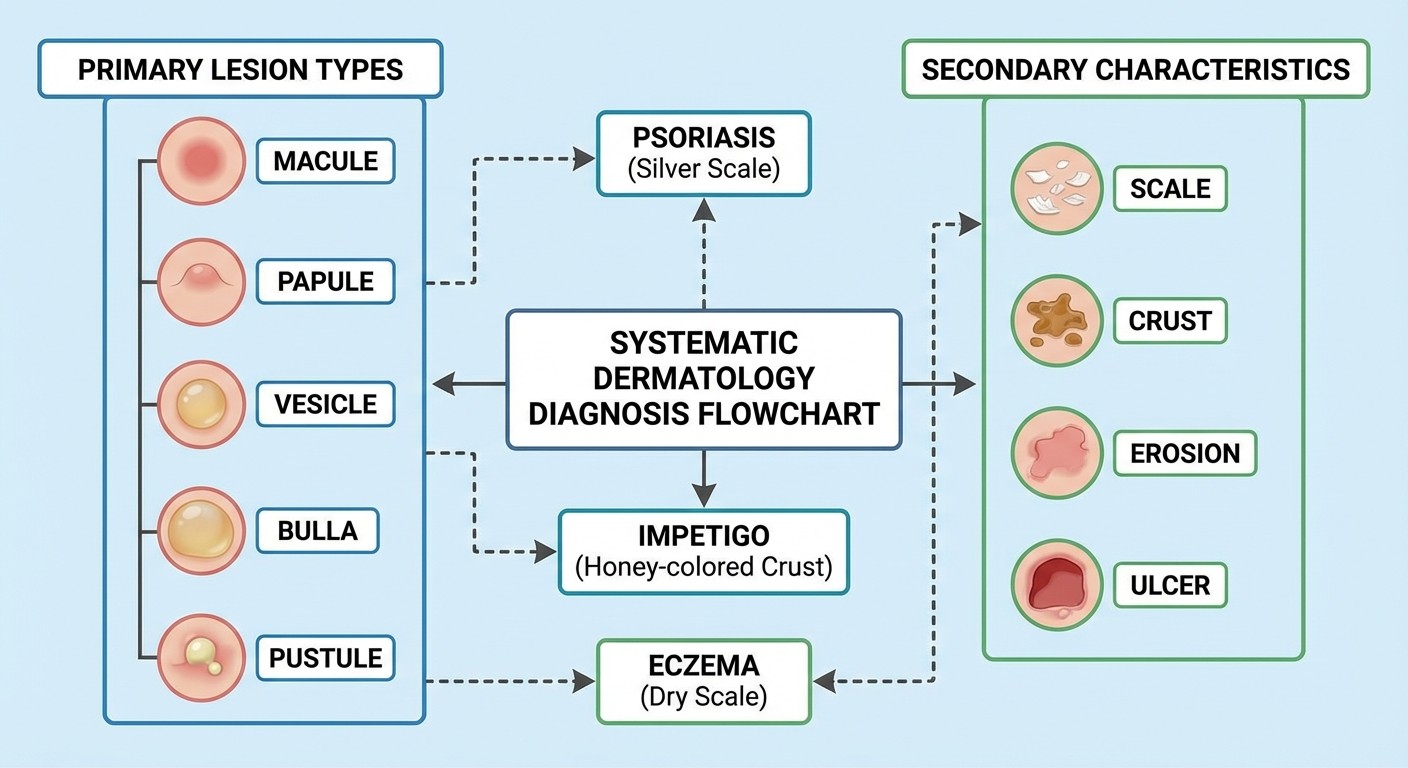
Primary Lesion Type: Macule (flat), papule (raised <5mm), plaque (raised >5mm), vesicle (fluid-filled <5mm), bulla (fluid-filled >5mm), pustule (pus-filled), or nodule (deep, >5mm). Distribution Pattern: Localized, generalized, symmetric, asymmetric, dermatomal, or following specific anatomic patterns. Secondary Changes: Scale, crust, erosion, ulceration, or lichenification from chronic scratching. Border Characteristics: Well-defined versus poorly demarcated edges.
Step 3: Generate Differential Diagnosis
Based on morphology and distribution, list 2-3 most likely diagnoses. Consider:
Inflammatory (psoriasis, eczema)
Infectious (bacterial, viral, fungal)
Neoplastic (benign vs malignant)
Autoimmune (pemphigus, lupus)
Step 4: Apply Clinical Context
Use patient factors to narrow your differential:
Age: Infantile eczema vs adult seborrheic dermatitis
Location: Face (seborrheic dermatitis, rosacea) vs hands (contact dermatitis, dyshidrotic eczema)
Chronicity: Acute (infection, contact) vs chronic (psoriasis, eczema)
Step 5: Consider Management
Step 2 CK often asks about next steps rather than diagnosis:
When to biopsy (any suspicious pigmented lesion)
First-line treatments (topical steroids for inflammatory conditions)
When to refer (rapid progression, systemic symptoms, uncertain diagnosis)
Dermatology Pharmacology High-Yield Facts
Understanding drug mechanisms and indications helps you tackle treatment questions confidently.
Topical Corticosteroids are first-line for most inflammatory skin conditions. Potency classification matters: low-potency (hydrocortisone) for face and intertriginous areas, high-potency (clobetasol) for thick plaques on body. Side effects include skin atrophy with prolonged use. Topical Calcineurin Inhibitors (tacrolimus, pimecrolimus) work for atopic dermatitis when steroids are contraindicated or cause atrophy. Black box warning for potential lymphoma risk, though clinical significance is debated. Systemic Antifungals treat severe or extensive fungal infections. Terbinafine is first-line for dermatophytes. Fluconazole works for Candida. Monitor liver function with prolonged use. Systemic Antibiotics target specific pathogens. Cephalexin or clindamycin for cellulitis. Doxycycline for atypical organisms or anti-inflammatory effects in rosacea. Biologic Agents represent newer therapies for severe psoriasis, atopic dermatitis, and other inflammatory conditions. TNF-alpha inhibitors (adalimumab) or IL-17 inhibitors (secukinumab) for psoriasis. Know that these increase infection risk and require screening for tuberculosis.
When studying pharmacology, focus on first-line agents and their specific indications. Oncourse performance analytics dashboard shows your accuracy across different drug categories — target your weak spots rather than reviewing everything equally.
When to Biopsy: Decision-Making Framework
Knowing when tissue diagnosis is needed separates good clinical reasoning from guessing.
Always Biopsy These Scenarios:
Any pigmented lesion concerning for melanoma (ABCDE criteria)
Persistent ulcers that dont heal within 4-6 weeks
New growths in elderly patients, especially on sun-exposed areas
Any lesion with rapid growth or bleeding
Bullous diseases to differentiate pemphigus from pemphigoid
Clinical Diagnosis Often Sufficient:
Classic psoriatic plaques with typical distribution
Clear infectious patterns (impetigo, cellulitis, tinea)
Common inflammatory conditions (atopic dermatitis, contact dermatitis)
Seborrheic keratoses with typical "stuck-on" appearance
Biopsy Technique Matters:
Shave biopsy for superficial lesions (seborrheic keratoses, basal cell carcinoma)
Punch biopsy for inflammatory conditions or deep lesions
Excisional biopsy for suspected melanoma (never shave a pigmented lesion)
The decision often depends on diagnostic certainty. When the clinical presentation clearly fits a benign condition and the patient has typical risk factors, observation and treatment trials are reasonable. Uncertainty or concerning features warrant tissue diagnosis.
Inflammatory vs Infectious vs Neoplastic: Quick Differentiation
Pattern recognition helps you categorize lesions quickly and focus your differential diagnosis.
Inflammatory Patterns
Bilateral, symmetric distribution (psoriasis, atopic dermatitis)
Chronic, waxing-waning course with stress or seasonal triggers
Response to anti-inflammatory treatments (topical steroids)
Associated with other inflammatory conditions (arthritis with psoriasis)
Infectious Patterns
Acute onset with rapid progression
Asymmetric, localized distribution following exposure patterns
Systemic symptoms (fever, malaise) in bacterial infections
Vesicular patterns in viral infections (herpes, varicella)
Neoplastic Patterns
Progressive growth without spontaneous resolution
Irregular morphology (asymmetric, irregular borders)
Age-related occurrence (increasing incidence with advanced age)
Sun-exposure correlation for skin cancers
This framework isn't absolute — some conditions blur categories. Seborrheic dermatitis is inflammatory but can have infectious components (Malassezia overgrowth). Chronic wounds may develop secondary bacterial infections. Use the predominant pattern to guide initial thinking, then refine based on specific features.
Common Dermatology Mistakes to Avoid
Learning from typical errors saves points on exam day.
Mistake 1: Confusing Psoriasis and Eczema
Psoriasis has well-demarcated plaques with silvery scale on extensor surfaces. Eczema shows poorly defined, pruritic patches in flexural areas with lichenification from scratching. When in doubt, look at the borders and distribution.
Mistake 2: Missing Melanoma Red Flags
Any pigmented lesion with asymmetry, irregular borders, color variation, diameter >6mm, or recent changes needs biopsy. Don't be falsely reassured by young age — melanoma can occur in patients under 30, especially with family history or multiple atypical nevi.
Mistake 3: Overusing Systemic Antibiotics for Cellulitis
Not every red, warm area needs antibiotics. Stasis dermatitis, contact dermatitis, and other inflammatory conditions can mimic cellulitis. Look for fever, lymphangitis, or systemic symptoms to support bacterial infection.
Mistake 4: Ignoring Drug Eruptions
Always review medication timeline when evaluating new rashes. Drug eruptions can mimic virtually any skin condition. Common culprits include antibiotics, anticonvulsants, and NSAIDs. Timing usually correlates with drug initiation.
Mistake 5: Forgetting Systemic Associations
Skin often reflects internal disease. Acanthosis nigricans suggests insulin resistance. Pyoderma gangrenosum associates with inflammatory bowel disease. Dermatomyositis may indicate underlying malignancy. Consider systemic workup for certain skin findings.
Study Timeline and Strategy
8-12 Weeks Before Exam
Start with foundational concepts. Review basic lesion morphology, primary skin diseases, and treatment categories. Use dermatology lessons to build systematic knowledge rather than memorizing random facts.
Focus on inflammatory conditions first (psoriasis, eczema, contact dermatitis) since these appear most frequently. Learn the pathophysiology — understanding why lesions occur in specific distributions helps with atypical presentations.
4-6 Weeks Before Exam
Shift to high-yield infectious conditions and skin cancers. Practice recognizing viral exanthems, bacterial infections, and fungal patterns. Study melanoma and non-melanoma skin cancers with emphasis on when to biopsy.
Add dermatology questions to your daily practice. Start with 10-15 questions per day, focusing on systematic approach rather than speed.
2-4 Weeks Before Exam
Integrate dermatology into your clinical scenarios. Many questions combine skin findings with internal medicine, pediatrics, or surgery. Practice multisystem questions where dermatology provides diagnostic clues.
Review dermatology flashcards daily using spaced repetition. Focus on high-yield facts like first-line treatments, biopsy indications, and systemic associations.
Final 1-2 Weeks
Perfect your timing and decision-making. Take timed dermatology question sets, aiming for 90 seconds per question. Review missed questions immediately to identify knowledge gaps versus careless errors.
Create a quick reference sheet with high-yield conditions, classic presentations, and first-line treatments. This reinforces key concepts without introducing new information.
Practice Question Approach
When practicing dermatology questions, use this systematic method:
1. Read the vignette thoroughly before looking at the image
2. Extract key clinical data: age, location, duration, symptoms
3. Examine the image systematically: morphology, distribution, secondary changes
4. Generate 2-3 differential diagnoses based on patterns
5. Apply clinical context to narrow choices
6. Select the best answer using evidence-based reasoning
7. Review explanations for both correct and incorrect choices
After each practice session, Oncourse performance analytics dashboard shows your accuracy by topic area — use this data to identify whether you need more work on infectious diseases, neoplasms, or inflammatory conditions rather than studying everything equally.
Track common mistake patterns. Are you missing questions because of poor image interpretation, inadequate clinical reasoning, or knowledge gaps? Target your weak areas specifically rather than general review.
Frequently Asked Questions
How Many Dermatology Questions Are on Step 2 CK?
Expect 15-20 dermatology questions spread throughout your 8-hour exam. These may appear in any block and often integrate with other specialties. Some questions focus purely on dermatology diagnosis and management, while others use skin findings as clues for systemic diseases.
Should I Memorize Every Skin Condition?
No. Focus on the 20-30 high-yield conditions that appear repeatedly. Master the systematic approach to skin lesion evaluation rather than memorizing rare diseases. Step 2 CK tests clinical reasoning more than encyclopedic knowledge.
How Important Are Images vs Text in Dermatology Questions?
Both matter equally. Many students focus only on images and miss crucial clinical context from the text. Age, location, duration, associated symptoms, and medical history often provide more diagnostic information than the image alone.
What's the Best Way to Study Dermatology Pharmacology?
Learn by mechanism and indication rather than memorizing drug lists. Understand when to use topical vs systemic therapy, steroid potency classifications, and major side effects. Focus on first-line treatments for common conditions.
How Do I Improve at Recognizing Skin Lesions?
Practice systematic image analysis daily. Use the morphology-first approach: identify primary lesion type, then secondary changes, then distribution pattern. Correlate images with clinical descriptions to build pattern recognition skills.
When Should I Seek Help With Dermatology Questions?
If your accuracy remains below 70% after dedicated study, you may need additional resources or teaching. Consider dermatology atlases, online question banks with detailed explanations, or tutoring focused on image interpretation skills.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.