Back
INICET Hematology Pharmacology Glossary 2026: Anticoagulants, Antiplatelets, Thrombolytics and Iron Therapy — High-Yield Drug Classes and MCQ Mnemonics
Master INICET hematology pharmacology with this comprehensive glossary covering anticoagulants, antiplatelets, thrombolytics, and iron therapy. Includes high-yield MCQ mnemonics and clinical pearls.

INICET Hematology Pharmacology Glossary 2026: Anticoagulants, Antiplatelets, Thrombolytics and Iron Therapy — High-Yield Drug Classes and MCQ Mnemonics
You are probably staring at your pharmacology notes thinking: "How am I supposed to remember 30+ hematology drugs, their mechanisms, reversals, and side effects for INICET?" Here's the reality — INICET hematology pharmacology questions test just 4 major drug classes, but they test them ruthlessly. One question asks about heparin reversal, the next about warfarin interactions, then aspirin resistance, then streptokinase contraindications.
INICET loves testing drug comparisons. UFH vs LMWH. Warfarin vs DOACs. Aspirin vs clopidogrel. Streptokinase vs alteplase. The examiners want to see if you can pick the right drug for the right patient in the right clinical scenario. This glossary covers exactly that — the 4 highest-yield drug classes with INICET-specific MCQ mnemonics and clinical pearls that actually show up in the exam.
Why These 4 Drug Classes Matter for INICET
INICET hematology pharmacology follows a predictable pattern. About 60% of questions come from anticoagulants and antiplatelets combined. Another 25% from thrombolytics. The remaining 15% from iron therapy and miscellaneous blood-related drugs. When you master these 4 classes, you have covered 85% of possible INICET hematology pharmacology MCQs.
The twist? INICET doesn't ask basic MOA questions. They test clinical applications, drug interactions, reversals, and side effects. A typical question: "A 65-year-old patient on warfarin presents with INR 8.5 and minor bleeding. Best immediate management?" The answer isn't warfarin MOA — it's knowing that vitamin K 2.5mg PO is preferred over FFP for minor bleeding with INR 5-10.
Anticoagulants: The High-Yield Quartet
Heparin Family: UFH vs LMWH
Unfractionated Heparin (UFH)
Mechanism: Binds antithrombin III → inactivates factors IIa (thrombin) and Xa
Route: IV/SC only
Monitoring: aPTT (target 1.5-2.5x normal)
Reversal: Protamine sulfate (1mg per 100 units of heparin)
Half-life: 1-2 hours
Low Molecular Weight Heparin (LMWH) - Enoxaparin
Mechanism: Primarily anti-Xa activity (less anti-IIa than UFH)
Route: SC only
Monitoring: Anti-Xa levels (usually not needed)
Reversal: Protamine partially effective (60-80%)
Half-life: 4-6 hours
INICET Mnemonic - "HEPARIN Monitoring":
Half-life: UFH short, LMWH long
Elimination: UFH renal+hepatic, LMWH renal
Partial reversal: LMWH with protamine
APTT monitoring: UFH yes, LMWH no
Renal adjustment: LMWH needs, UFH doesn't
IV possible: UFH yes, LMWH no
Neutralizable: UFH completely, LMWH partially
For students working through hematology MCQs, every question about heparin reversal gets an AI explanation covering why protamine works for UFH but only partially for LMWH — turning each attempt into active pharmacology learning.
Warfarin: The Vitamin K Antagonist
Mechanism: Inhibits vitamin K epoxide reductase → blocks synthesis of factors II, VII, IX, X + proteins C & S Key Clinical Points:
Monitoring: INR (target varies by indication)
Onset: 48-72 hours (factor VII depleted first)
Peak effect: 5-7 days
Reversal: Vitamin K (PO/IV), FFP, PCC (Prothrombin Complex Concentrate)
Major Drug Interactions (INICET Favorites):
Potentiate warfarin (↑INR): Metronidazole, sulfamethoxazole, amiodarone, cimetidine, erythromycin
Antagonize warfarin (↓INR): Phenytoin, carbamazepine, rifampin, barbiturates
INICET Mnemonic - "WARFARIN Interactions":
Weakens with phenytoin/rifampin
Augmented by metronidazole/amiodarone
Rifampin reduces effect
Factors II, VII, IX, X blocked
Anticoagulation reversed by vitamin K
Requires 3-5 days to reach steady state
INR monitoring essential
Needs CYP2C9 metabolism
Direct Oral Anticoagulants (DOACs)
Rivaroxaban & Apixaban (Factor Xa Inhibitors)
Mechanism: Direct factor Xa inhibition
Monitoring: Not routinely needed
Reversal: Andexanet alfa (expensive), PCC as alternative
Advantages: Fixed dosing, fewer interactions
Dabigatran (Direct Thrombin Inhibitor)
Mechanism: Direct thrombin (factor IIa) inhibition
Monitoring: Not routinely needed
Reversal: Idarucizumab (specific antidote)
Renal elimination: 80% (requires dose adjustment in CKD)
Students using Synapses flashcards can save DOAC comparison tables for spaced repetition — essential for retaining the differences between rivaroxaban's once-daily dosing vs apixaban's twice-daily regimen before INICET.
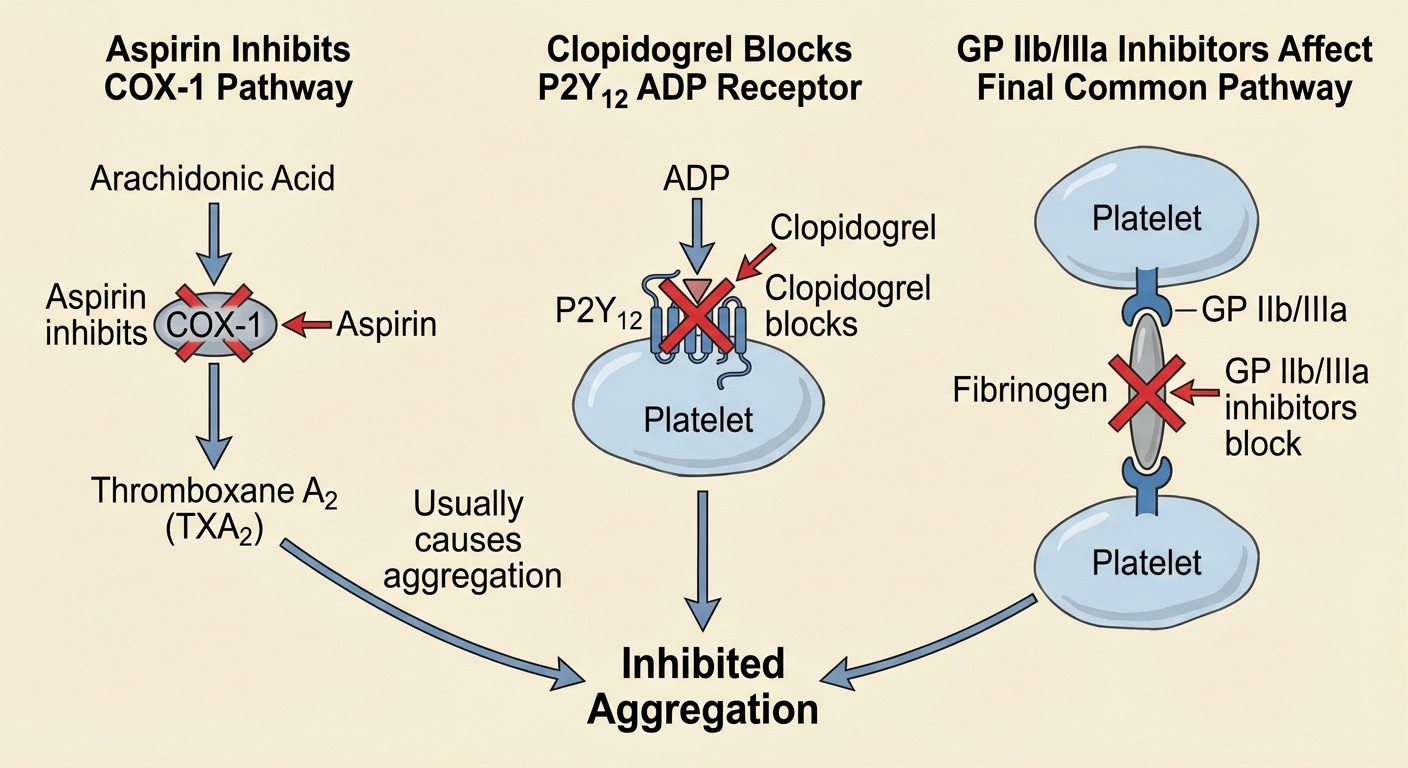
Antiplatelet Agents: Targeting Different Pathways
Aspirin: The COX-1 Inhibitor
Low-dose Aspirin (75-100mg)
Mechanism: Irreversibly inhibits COX-1 → blocks TXA2 synthesis → reduces platelet aggregation
Duration: Permanent (platelet lifespan 7-10 days)
Side effects: GI bleeding, tinnitus, Reye syndrome (children)
INICET Pearl: Aspirin resistance occurs in 10-15% patients. Alternative: clopidogrel, not higher aspirin dose.
P2Y12 Inhibitors: ADP Pathway Blockers
Clopidogrel
Mechanism: Irreversibly blocks P2Y12 ADP receptors
Onset: 4-6 hours (requires hepatic conversion to active metabolite)
Duration: 5-7 days
Key interaction: PPI (especially omeprazole) reduces efficacy
Ticagrelor
Mechanism: Reversibly blocks P2Y12 receptors
Onset: 30 minutes (no hepatic conversion needed)
Duration: 3-4 days
Side effect: Dyspnea (10-15% patients)
Prasugrel
Mechanism: Irreversibly blocks P2Y12 receptors
Onset: 15-30 minutes
Contraindication: History of stroke/TIA
Advantage: No CYP2C19 interaction (unlike clopidogrel)
INICET Mnemonic - "CLOPI-TICAGREL-PRASUGREL":
Clopidogrel: CYP2C19 dependent, PPI interaction
Lasting 5-7 days (irreversible)
Onset slow (4-6 hours)
Platelet function affected
Irreversible binding
Ticagrelor: Takes 30 minutes onset
Independent of CYP metabolism
Causes dyspnea
Active without conversion
Good in ACS
Reversible binding
Expires in 3-4 days
Less stroke risk than prasugrel
GP IIb/IIIa Inhibitors
Abciximab, Eptifibatide, Tirofiban
Mechanism: Block final common pathway of platelet aggregation
Use: IV only, acute settings (PCI, ACS)
Monitoring: Bleeding time, platelet count
Reversal: Platelet transfusion
Thrombolytic Agents: Clot Busters
Streptokinase
Mechanism: Activates plasminogen → plasmin → fibrin degradation INICET High-Yield Facts:
Antigenic: Can cause allergic reactions, antibody formation
Hypotension: Most common side effect (30-40% patients)
Contraindication: Previous streptokinase use (within 1 year), recent surgery
Cost: Cheapest thrombolytic
Alteplase (tPA)
Mechanism: Tissue plasminogen activator — fibrin-specific thrombolysis Advantages over streptokinase:
Non-antigenic: No allergic reactions
Fibrin-specific: Less systemic plasminogen activation
Faster: 90-minute vs 3-hour infusion
Efficacy: Better mortality reduction in STEMI
Tenecteplase: Single bolus version of alteplase, weight-based dosing INICET Mnemonic - "STREP vs tPA":
Strep causes allergies, tPA safe
Time: Strep 3 hours, tPA 90 minutes
Reactions: Strep antigenic, tPA not
Effectiveness: tPA superior
Price: Strep cheaper, tPA expensive
When working through anticoagulant pharmacology lessons, students often miss the streptokinase antigenicity concept. Oncourse's adaptive system automatically increases thrombolytic questions if you consistently miss this high-yield INICET pattern.
Common Thrombolytic Contraindications (INICET Traps)
Absolute Contraindications:
Active bleeding
Intracranial hemorrhage (any time)
Recent head trauma (<3 months)
Known intracranial neoplasm
Relative Contraindications:
Recent surgery (<14 days)
Uncontrolled hypertension (>180/110)
Active peptic ulcer disease
Pregnancy
Iron Therapy: Deficiency to Overload
Oral Iron Preparations
Ferrous Sulfate (Most Common)
Elemental iron: 20% (65mg elemental iron per 325mg tablet)
Absorption: Best on empty stomach, with vitamin C
Side effects: GI upset, constipation, dark stools
Interactions: Reduced by antacids, tea, calcium
Ferrous Fumarate: 33% elemental iron (highest concentration) Ferrous Gluconate: 12% elemental iron (best tolerated) INICET Pearl: Iron absorption increases 3-4 fold in iron deficiency. Normal absorption is only 5-10%.
Intravenous Iron
Iron Sucrose
Dose: 100-200mg per infusion
Frequency: 2-3 times per week
Side effects: Hypotension, anaphylaxis (rare)
Ferric Carboxymaltose
Advantage: Single large dose (up to 1000mg)
Onset: Faster than iron sucrose
Cost: More expensive
INICET Indications for IV Iron:
Severe iron deficiency (Hb <7 g/dL)
Oral iron intolerance
Malabsorption syndromes
Chronic kidney disease
Heart failure patients
Iron Chelation Therapy
Deferoxamine
Route: IV/SC infusion
Mechanism: Binds free iron → forms ferrioxamine → renal excretion
Side effects: Ototoxicity, retinal toxicity, growth retardation
Monitoring: Audiometry, ophthalmology exams
Deferasirox (Oral Chelator)
Advantage: Once daily oral dosing
Side effects: Nephrotoxicity, hepatotoxicity, GI upset
Monitoring: Creatinine, liver function tests
INICET Mnemonic - "IRON Chelation":
IV deferoxamine for acute poisoning
Renal toxicity with deferasirox
Oral deferasirox for chronic use
Needs monitoring (kidney, liver, eyes, ears)
Students can create iron therapy flashcards comparing oral vs IV preparations — crucial for remembering that ferrous fumarate has the highest elemental iron content but ferrous sulfate remains most commonly used.
INICET MCQ Traps and Clinical Pearls
Heparin-Induced Thrombocytopenia (HIT)
Type 1 HIT: Mild, transient thrombocytopenia within 2 days Type 2 HIT: Severe, paradoxical thrombosis + thrombocytopenia after 5-10 days Management: Stop heparin immediately, start argatroban or bivalirudin INICET Trap: Never use LMWH in HIT — cross-reactivity occurs in 80% cases
Warfarin Reversal Guidelines
INR Range | Bleeding | Management |
|---|---|---|
<5 | None | Hold warfarin, recheck INR |
5-9 | None/Minor | Vitamin K 2.5mg PO |
5-9 | Major | Vitamin K 10mg IV + FFP/PCC |
>9 | Any bleeding | Vitamin K 10mg IV + FFP/PCC |
Aspirin vs Clopidogrel Selection
Use Aspirin when:
Primary prevention (low bleeding risk)
Cost is a factor
No GI contraindications
Use Clopidogrel when:
Aspirin allergy/intolerance
High GI bleeding risk
Recent GI bleeding on aspirin
Streptokinase vs Alteplase in STEMI
Choose Streptokinase if:
Cost limitation
No previous streptokinase use
Patient hemodynamically stable
Choose Alteplase if:
Previous streptokinase use
Time-critical situation
High bleeding risk (fibrin-specific)
Advanced INICET Concepts
Dual Antiplatelet Therapy (DAPT) Duration
Post-PCI with stents:
Bare metal stents: 4 weeks minimum
Drug-eluting stents: 6-12 months standard
High bleeding risk: Shorter duration acceptable
INICET Question Pattern: They ask about optimal DAPT duration after presenting a patient with specific bleeding risk factors.
Anticoagulation in Special Populations
Pregnancy:
Safe: UFH, LMWH
Contraindicated: Warfarin (teratogenic), DOACs (unknown safety)
Renal Impairment:
Dose reduction needed: Dabigatran (80% renal excretion)
Minimal adjustment: Rivaroxaban, apixaban (25-35% renal excretion)
Liver Disease:
Avoid warfarin in severe hepatic impairment
DOACs relatively safer but use with caution
Frequently Asked Questions
What is the most common side effect of streptokinase?
Hypotension occurs in 30-40% of patients receiving streptokinase. This is why IV fluids are often co-administered during infusion. The mechanism involves kinins and complement activation leading to vasodilation.
When should you suspect heparin-induced thrombocytopenia?
Suspect HIT when platelet count drops >50% from baseline after 5-10 days of heparin therapy, especially if paradoxical thrombosis occurs. The 4T score helps assess probability: Thrombocytopenia severity, Timing, Thrombosis, and other causes.
Which oral iron preparation has the highest elemental iron content?
Ferrous fumarate contains 33% elemental iron, making it the highest among oral preparations. However, ferrous sulfate remains most commonly prescribed due to cost and availability, containing 20% elemental iron.
What is the reversal agent for dabigatran?
Idarucizumab is the specific reversal agent for dabigatran, neutralizing its anticoagulant effect within minutes. For other DOACs (rivaroxaban, apixaban), andexanet alfa is used, though prothrombin complex concentrate (PCC) serves as an alternative.
Can LMWH be used in patients with heparin-induced thrombocytopenia?
No, LMWH should never be used in HIT due to 80% cross-reactivity with UFH antibodies. Alternative anticoagulants include argatroban, bivalirudin, or fondaparinux.
Why is vitamin C given with iron supplements?
Vitamin C (ascorbic acid) reduces ferric iron (Fe3+) to ferrous iron (Fe2+), which is the absorbable form. This can increase iron absorption by 3-4 fold, especially important in iron deficiency anemia treatment.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for INICET. Download free on Android and iOS.