Back
Sentinel Lymph Node Biopsy in Breast Cancer: Surgery High-Yield Guide for NEET PG and USMLE (2026)
Master sentinel lymph node biopsy for NEET PG and USMLE. Complete guide covering indications, technique, adverse reactions, and clinical scenarios including the classic 1cm IDC case.

Sentinel Lymph Node Biopsy in Breast Cancer: Surgery High-Yield Guide for NEET PG and USMLE (2026)
You are staring at a 40-year-old woman with a 1cm infiltrating ductal carcinoma. Clinically node-negative. The question asks: what is the appropriate axillary staging procedure? If you picked "axillary lymph node dissection," you just lost 4 marks. The correct answer is sentinel lymph node biopsy (SLNB) — and understanding why separates the toppers from the rest.
NEET PG loves testing SLNB because it perfectly combines anatomy, physiology, and surgical decision-making. The examiners know most students memorize "SLNB for early breast cancer" without understanding the nuances. They test the contraindications, adverse reactions to blue dye, and what happens when the sentinel node is positive.
This is your complete guide to mastering sentinel lymph node biopsy for both NEET PG and USMLE Step 2. We'll cover the high-yield MCQ patterns, clinical scenarios, and the exact decision trees you need to ace every question.
What is Sentinel Lymph Node Biopsy?
The sentinel lymph node is the first lymph node that receives lymphatic drainage from a primary tumor. In breast cancer, this concept revolutionized axillary staging because if the sentinel node is negative for metastases, the remaining axillary lymph nodes are highly unlikely to contain cancer cells (negative predictive value >95%).
SLNB involves identifying and removing 1-3 sentinel lymph nodes for histopathological examination. This minimally invasive procedure has largely replaced routine axillary lymph node dissection (ALND) for early-stage breast cancer patients.
Why SLNB Matters for Your Exam
NEET PG and USMLE consistently test SLNB because it demonstrates:
Surgical anatomy (lymphatic drainage patterns)
Evidence-based medicine (replacing more extensive surgery)
Risk-benefit analysis (minimizing morbidity while maintaining accuracy)
Clinical decision-making (when to proceed vs when to avoid)
The key insight: SLNB is not just a technical procedure — it's a staging tool that guides further treatment decisions.
Indications for Sentinel Lymph Node Biopsy
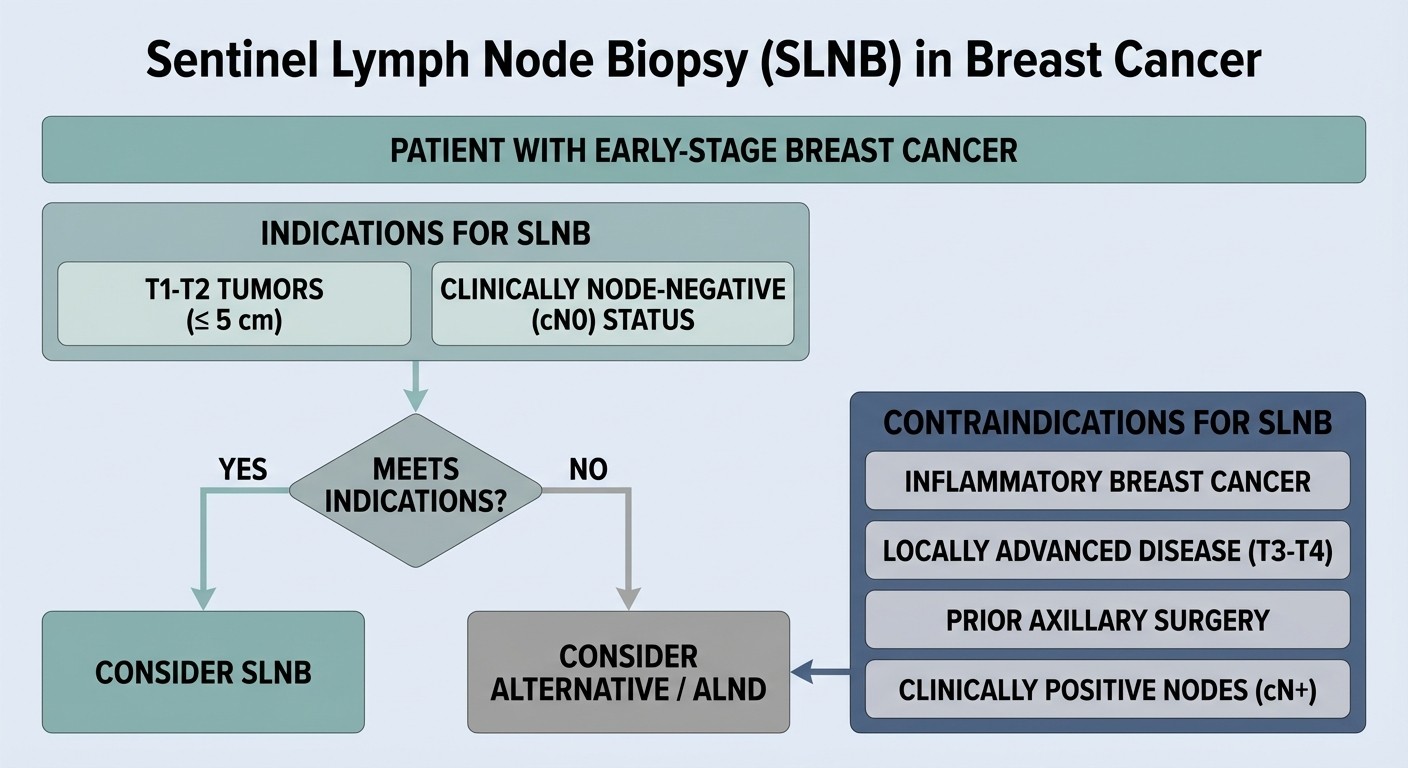
Primary Indications
1. Clinically Node-Negative Early Breast Cancer
T1 tumors (≤2 cm)
T2 tumors (2.1-5 cm) without clinical or radiological evidence of axillary involvement
Both invasive ductal carcinoma (IDC) and invasive lobular carcinoma (ILC)
2. Ductal Carcinoma in Situ (DCIS)
Only when mastectomy is planned
High-grade DCIS with suspicious features
DCIS ≥5 cm or when upstaging to invasive cancer is suspected
3. Special Situations
Multifocal disease (multiple tumors in same quadrant) if largest lesion meets criteria
After neoadjuvant chemotherapy (if initially node-negative)
Recurrent breast cancer in previously untreated axilla
High-Yield NEET PG Pattern
The classic NEET PG question presents a 40-year-old woman with 1cm infiltrating ductal carcinoma, clinically node-negative on examination and imaging. The correct axillary staging procedure is SLNB, not routine ALND.
Why this matters: Students often confuse "small tumor = less surgery" with the actual indication criteria. Size matters, but clinical node status is equally crucial.
Contraindications to SLNB
Understanding contraindications is where most students lose marks. These are absolute deal-breakers:
Absolute Contraindications
1. Clinically Positive Axillary Nodes
Palpable, suspicious lymph nodes
Radiologically suspicious nodes (FNA/core biopsy positive)
Fixed or matted axillary lymphadenopathy
2. Inflammatory Breast Cancer
Skin changes (peau d'orange, erythema, induration)
Rapid onset of symptoms
Dermal lymphatic invasion on biopsy
3. Previous Axillary Surgery
Prior ALND or extensive axillary intervention
Disrupted lymphatic drainage patterns
4. Pregnancy
Radiotracer contraindicated
Blue dye crosses placenta
Relative Contraindications
Large tumors (>5 cm) — higher false-negative rates
Multicentric disease (tumors in different quadrants)
Prior excisional biopsy with extensive disruption
Severe medical comorbidities
NEET PG Trap: The question may describe a patient with "mobile, non-tender axillary lymph nodes" — this doesn't automatically mean SLNB is contraindicated. You need tissue confirmation (FNA/core biopsy) of malignancy before calling nodes "clinically positive."
SLNB Technique: Blue Dye + Radiotracer Method
The dual-agent technique using blue dye and technetium-99m labeled sulfur colloid is the gold standard. Understanding both components is essential for exam questions.
Step-by-Step Procedure
1. Preoperative Preparation
Technetium-99m sulfur colloid injection 1-6 hours before surgery
Periareolar, peritumoral, or intradermal injection
Lymphoscintigraphy to map drainage patterns
2. Intraoperative Blue Dye
Isosulfan blue or methylene blue injection
2-5 mL periareolar or peritumoral
10-15 minutes before incision for optimal uptake
3. Identification and Removal
Gamma probe detection of radioactive nodes
Visual identification of blue-stained lymphatics and nodes
Remove all hot and/or blue nodes
Typical yield: 1-3 sentinel lymph nodes
Why Dual-Agent Technique?
Blue dye alone: 84% identification rate
Radiotracer alone: 92% identification rate
Combined technique: 97-99% identification rate
The redundancy ensures you dont miss the sentinel node, which would compromise staging accuracy.
Adverse Reactions to Blue Dye: High-Yield NEET PG Topic
This is a favorite NEET PG MCQ topic because adverse reactions to blue dye are well-documented, predictable, and clinically significant.
Types of Adverse Reactions
1. Allergic Reactions (Most Important for Exams)
Mild: Skin rash, urticaria, localized swelling
Moderate: Bronchospasm, hypotension
Severe: Anaphylactic shock, cardiovascular collapse
Incidence: 1-3% of patients receiving isosulfan blue Risk factors: Previous exposure to blue dye, history of drug allergies 2. Non-Allergic Reactions
Blue discoloration of skin and urine (lasts 24-48 hours)
Temporary tattooing at injection site
Interference with pulse oximetry readings
NEET PG High-Yield Fact
Question pattern: "A 45-year-old woman develops hypotension and bronchospasm 15 minutes after blue dye injection during SLNB. What is the most likely cause?" Answer: Anaphylactic reaction to isosulfan blue dye Management: Immediate IV epinephrine, corticosteroids, antihistamines, supportive care Prevention: Detailed allergy history, premedication in high-risk patients, alternative agents (methylene blue has lower allergy rates)
What Happens After SLNB: The Decision Tree
The sentinel lymph node result determines the next surgical step. This is where clinical decision-making becomes crucial for exam questions.
If Sentinel Lymph Node is Negative
No further axillary surgery required
Proceed with planned breast surgery (lumpectomy or mastectomy)
Standard adjuvant therapy based on tumor characteristics
False negative rate: <5% with proper technique
If Sentinel Lymph Node is Positive
The management depends on several factors:
1. Completion Axillary Lymph Node Dissection (cALND) Indications for cALND:
Mastectomy planned
>2 positive sentinel lymph nodes
Extracapsular extension in sentinel node
Large volume metastases (>2 mm)
2. Avoid cALND (Watchful Waiting) Based on ACOSOG Z0011 Trial:
Lumpectomy with whole breast radiation planned
1-2 positive sentinel lymph nodes
No extracapsular extension
No additional high-risk features
NEET PG Clinical Scenario Breakdown
Case: 40-year-old woman with 1cm IDC, clinically node-negative. SLNB shows 1 positive sentinel lymph node with microscopic disease. She's planned for lumpectomy and radiation. Question: What is the next appropriate step? Answer: Proceed with lumpectomy and radiation — completion ALND not required Rationale: ACOSOG Z0011 trial showed no survival difference between cALND and observation in this specific scenario.
Clinical Scenario Mastery: The 1cm IDC Case
Let's break down the classic NEET PG clinical scenario that this article specifically targets.
The Setup
"A 40-year-old woman presents with a 1cm infiltrating ductal carcinoma of the left breast. Physical examination reveals no palpable axillary lymph nodes. Mammography and ultrasound show no suspicious axillary adenopathy. What is the appropriate axillary staging procedure?"
The Analysis
Key decision points: 1. Tumor size: 1cm = T1 tumor (eligible for SLNB) 2. Clinical node status: Negative (no palpable nodes + negative imaging) 3. Histology: Infiltrating ductal carcinoma (standard indication) 4. Patient factors: No mentioned contraindications Correct answer: Sentinel lymph node biopsy Why not axillary lymph node dissection?
Unnecessary morbidity for clinically node-negative disease
SLNB provides equivalent staging information
Lower risk of lymphedema, shoulder dysfunction
Common NEET PG Distractors
"Fine needle aspiration of axillary lymph nodes" — Wrong because nodes are clinically negative
"CT scan of chest and abdomen" — Not part of axillary staging
"Prophylactic axillary radiation" — Not standard of care
"Observation without staging" — Inadequate staging for invasive cancer
SLNB vs Axillary Lymph Node Dissection: When Each is Appropriate
Understanding the evolution from ALND to SLNB helps you answer comparison questions correctly.
Historical Context
Before SLNB, all breast cancer patients underwent routine ALND for staging. This caused significant morbidity:
Lymphedema rates: 20-30%
Shoulder dysfunction: 15-25%
Chronic pain and numbness
SLNB reduced these complications while maintaining staging accuracy.
Current Decision Algorithm
Clinical Scenario | Appropriate Procedure | Rationale |
|---|---|---|
T1-T2, cN0 (clinically node-negative) | SLNB | Standard of care, minimal morbidity |
cN1-N2 (clinically node-positive) | ALND | Skip SLNB, proceed to definitive staging |
SLNB positive, mastectomy planned | cALND | Complete staging required |
SLNB positive, lumpectomy + XRT planned | Consider observation | Based on Z0011 criteria |
High-Yield NEET PG MCQ Patterns
Based on previous year analysis, these are the most frequently tested SLNB concepts:
Pattern 1: Indication Selection
Question type: Clinical vignette → choose appropriate staging procedure Key variables: Tumor size, clinical node status, patient factors Common trap: Picking ALND for small tumors or SLNB for node-positive disease
Pattern 2: Adverse Reactions
Question type: Intraoperative complication → identify cause and management Focus: Anaphylactic reaction to blue dye Key fact: 1-3% incidence with isosulfan blue
Pattern 3: Post-SLNB Management
Question type: SLNB results → determine next surgical step Critical knowledge: Z0011 trial criteria for avoiding completion ALND Trap: Reflexively choosing cALND for any positive sentinel node
Pattern 4: Technical Details
Question type: Procedure specifics → dual-agent technique, timing, identification rates High-yield facts: 97-99% identification with dual agents, false-negative rate <5%
How Oncourse AI Covers Breast Surgery Systematically
Understanding how Oncourse structures breast surgery content helps you learn more efficiently. Our platform breaks down complex surgical topics into digestible, exam-focused modules.
SLNB Learning Path on Oncourse
1. Fundamental breast surgery lessons — Basic anatomy and physiology
2. SLNB technique modules — Step-by-step procedural details
3. Clinical decision-making scenarios — Practice with real exam-style MCQs
4. Complication management — Adverse reactions and troubleshooting
Oncourse's Systematic Approach
Spaced repetition flashcards help you memorize contraindications and indications
AI-powered explanations break down why wrong answers are incorrect
Progressive difficulty — start with basic concepts, advance to complex clinical scenarios
Cross-linking — connects SLNB to related topics like axillary anatomy and breast cancer staging
The platform's strength is connecting isolated facts into clinical reasoning patterns. Instead of memorizing "SLNB for T1-T2 cN0," you learn the complete decision tree including what happens when sentinel nodes are positive.
Practice with Oncourse breast surgery questions to reinforce these concepts systematically.
Advanced SLNB Concepts for USMLE Step 2
USMLE tends to test more nuanced scenarios and recent research developments.
Neoadjuvant Chemotherapy and SLNB
Key concept: SLNB after neoadjuvant chemotherapy has higher false-negative rates Current practice:
If initially node-negative → SLNB acceptable after neoadjuvant therapy
If initially node-positive → ALND recommended regardless of response
Molecular Markers and SLNB
Intraoperative assessment:
Frozen section analysis during surgery
Molecular assays (GeneSearch, OSNA) for rapid results
Helps decide on immediate completion ALND vs staged procedure
Quality Metrics
USMLE may test:
Identification rate targets: >95%
False-negative rate goals: <5%
Learning curve requirements: 20-30 cases for competency
Future Directions and Controversies
Ongoing Clinical Trials
SOUND trial: Evaluating omission of SLNB in elderly patients with low-risk tumors
SENOMAC trial: SLNB vs no axillary surgery in select patients
Areas of Active Research
Circulating tumor DNA as alternative to surgical staging
Advanced imaging techniques (PET-MRI) for non-invasive node assessment
Expanded criteria for avoiding completion ALND
Frequently Asked Questions
Is SLNB appropriate for a 35-year-old woman with 2.5cm IDC and clinically negative axilla?
Yes. The tumor is T2 (2.1-5cm) and clinically node-negative, meeting standard SLNB criteria. Size alone doesn't preclude SLNB unless >5cm.
What if the patient has a history of allergic reactions to contrast agents?
Inform the anesthesiologist and surgeon. Consider premedication with steroids and antihistamines. Methylene blue has lower allergy rates than isosulfan blue. Have emergency medications readily available.
Can SLNB be performed during pregnancy?
No. The radiotracer (technetium-99m) crosses the placenta and is contraindicated. Blue dye also crosses the placental barrier. Defer SLNB until after delivery if possible.
If 3 sentinel lymph nodes are identified and 2 are positive, what's the next step?
This depends on the planned breast surgery. If mastectomy is planned, proceed with completion ALND. If lumpectomy with radiation is planned, completion ALND is typically recommended for >2 positive nodes.
What is the false-negative rate of SLNB?
The false-negative rate is <5% when performed by experienced surgeons using dual-agent technique. This means <5% of patients with negative SLNB actually have positive non-sentinel nodes.
How long does blue discoloration last after methylene blue injection?
Skin and urine discoloration typically resolves within 24-48 hours. Patients should be warned about this cosmetic effect, especially the blue-green urine color that can be alarming if unexpected.
---
Sentinel lymph node biopsy represents the evolution of surgical oncology — less invasive procedures with equivalent outcomes. Master the indications, contraindications, and decision trees, and you'll handle any SLNB question on NEET PG or USMLE with confidence.
The key insight is recognizing SLNB as a staging tool, not just a surgical procedure. It's the bridge between clinical assessment and definitive treatment planning.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG and USMLE. Download free on Android and iOS.