Back
MRCP Preparation 2026: Complete Study Guide for Part 1, Part 2 Written and PACES
Master MRCP 2026 with our integrated approach to Part 1, Part 2 Written, and PACES. Stop preparing for three exams, start preparing for one medical career with proven strategies.

MRCP Preparation 2026: Complete Study Guide for Part 1, Part 2 Written and PACES
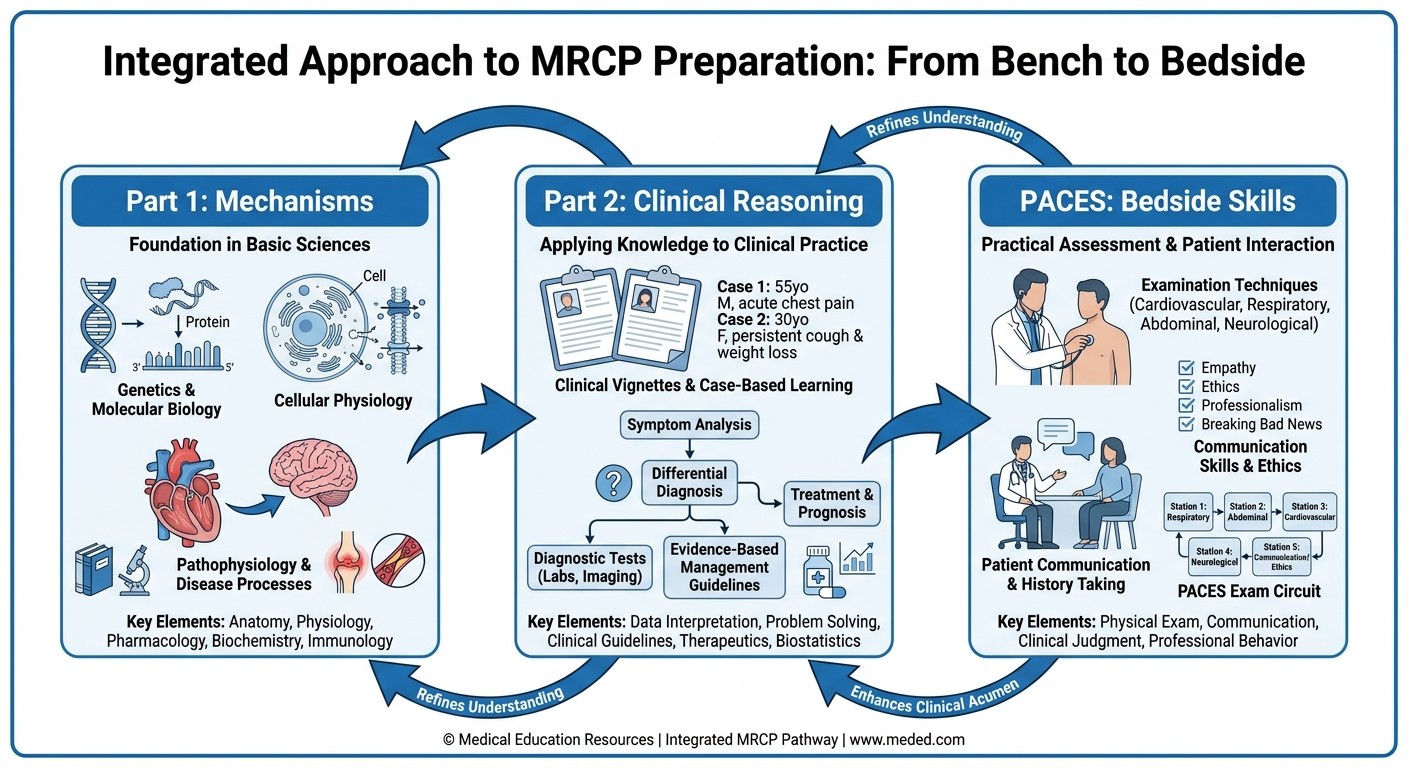
You have spent months staring at the MRCP application page. Part 1, Part 2 Written, PACES — three exams that feel like three different careers. Most candidates prepare for each stage in isolation, burning through resources and time. Here's what they miss: MRCP isnt three separate exams. Its one integrated assessment of clinical competency that builds from basic science through clinical reasoning to bedside skills.
The doctors who clear MRCP on their first attempt understand this. They dont prepare for three exams — they prepare for one medical career. This guide shows you how to build that integrated knowledge base and leverage it across all three stages, cutting your preparation time while improving your pass probability.
By the end of this guide, you will have a clear roadmap for mastering the 2026 MRCP pathway, from Part 1's basic science foundations through Part 2's clinical vignettes to PACES' practical skills — all as one coherent preparation strategy.
Understanding MRCP 2026: What Really Matters
The MRCP (UK) remains the gold standard for postgraduate medical training across the UK and internationally. In 2026, the exam structure continues with three distinct components, but understanding how they interconnect is what separates successful candidates from those who struggle.
The Three-Stage Structure:
Part 1: Two 3-hour papers, 100 single best answer (SBA) questions each
Part 2 Written: Two 3-hour papers, 100 SBA questions each, clinically focused
PACES: Five 20-minute stations testing clinical examination and communication skills
Here's the key insight most prep guides miss: Part 1 tests the physiological and pharmacological foundations you need for Part 2's clinical reasoning. Part 2's evidence-based medicine and clinical decision-making directly feeds into PACES' consultation and communication stations. Master the connections, and you prepare for one exam instead of three.
2026 Changes You Need to Know:
Starting in 2026, MRCP written examinations move from remote online proctoring back to in-centre computer-based testing. This improves exam security and reduces technical issues that plagued remote delivery. PACES continues its established five-station format introduced in 2023, with pass rates ranging from 50-77% depending on your timing post-graduation.
Part 1 Preparation: Building Your Clinical Foundation
Part 1 isnt about memorizing facts — its about understanding mechanisms that explain clinical presentations. The exam tests basic science through clinical scenarios, and your approach should reflect this integration.
High-Yield Subject Breakdown
Cardiology (15-20 questions)
Focus on pathophysiology that explains clinical findings. Heart failure progression from compensated to decompensated states. Arrhythmia mechanisms that inform ECG interpretation. Valvular disease hemodynamics that predict examination findings.
For systematic review of cardiac physiology and pathology, explore our comprehensive cardiology lessons. The key is understanding how molecular mechanisms scale up to bedside findings you'll encounter in PACES.
Respiratory Medicine (12-15 questions)
Ventilation-perfusion matching, gas exchange, and spirometry interpretation form the foundation. COPD pathophysiology, asthma mechanisms, and pneumonia management guidelines are heavily tested. Understanding oxygen delivery and CO2 elimination prepares you for respiratory station encounters in PACES.
Practice with our respiratory medicine question bank to reinforce pattern recognition between basic science and clinical presentations.
Clinical Pharmacology (15-18 questions)
This is where integration pays off. Drug mechanisms of action predict both therapeutic effects and adverse reactions. Beta-blocker selectivity explains why propranolol is contraindicated in asthma while bisoprolol might be acceptable. ACE inhibitor mechanisms predict both their cardiac benefits and risk of hyperkalemia.
When studying pharmacology tables, dont just memorize — understand why each drug works and fails. For spaced repetition of drug mechanisms and interactions, Oncourse's Synapses flashcards can help you retain complex pharmacokinetic relationships without endless rereading.
Neurology (8-12 questions)
Anatomy-based reasoning dominates here. Understanding corticospinal tract anatomy explains upper motor neuron signs. Cranial nerve pathways predict examination findings. Neurotransmitter systems inform both pathophysiology and pharmacological interventions.
The neurological examination stations in PACES directly test the anatomical knowledge from Part 1. When you study cerebellar pathways, visualize how cerebellar dysfunction presents during the coordination tests you'll perform at the neurology station.
Other High-Yield Areas:
Endocrinology: Hormone axis regulation, diabetes pathophysiology, thyroid disorders
Renal Medicine: Fluid and electrolyte balance, acid-base disorders, glomerular disease
Hematology: Coagulation cascades, anemia classification, hematological malignancies
Infectious Diseases: Antimicrobial mechanisms, resistance patterns, immunocompromised hosts
Part 1 Study Strategy
Phase 1 (Weeks 1-4): Foundation Building
Start with physiology and pathology. Use a systematic approach — cardiovascular week 1, respiratory week 2, renal week 3, neurological week 4. For each system, master normal physiology first, then understand how disease disrupts normal function.
Phase 2 (Weeks 5-8): Integration and Application
Move to question-based learning. Target 30-40 questions daily, focusing on explanation analysis. When you get a question wrong, dont just read the correct answer — understand why the incorrect options are wrong and what clinical principle they test.
Phase 3 (Weeks 9-12): Consolidation and Speed
Full-length mock examinations under timed conditions. Aim for 1.8 minutes per question average. Build stamina for the 3-hour paper duration. Track performance by subject to identify persistent weaknesses.
Part 2 Written: Clinical Reasoning Under Pressure
Part 2 Written separates memorizers from clinicians. Success requires applying basic science knowledge to complex clinical scenarios, often with incomplete information and time pressure. The exam tests clinical decision-making, not recall.
Question Pattern Analysis
Clinical Vignettes (70-80% of questions)
These present patient scenarios requiring diagnosis, investigation, or management decisions. Unlike Part 1's mechanism-focused questions, Part 2 tests your clinical judgment. You might see a 68-year-old with chest pain, elevated troponin, and new LBBB — the question tests whether you recognize STEMI equivalent and choose primary PCI over thrombolysis.
Evidence-Based Medicine (15-20% of questions)
Study design, statistical interpretation, and guideline application appear regularly. Understanding number needed to treat, likelihood ratios, and confidence intervals is essential. These arent abstract concepts — they inform the treatment recommendations you'll make in PACES consultations.
For comprehensive coverage of evidence-based medicine principles, review our EBM lessons which translate statistical concepts into clinical decision-making.
Imaging and Investigation Interpretation (5-10% of questions)
ECGs, chest X-rays, and basic imaging interpretation appear integrated within clinical vignettes. The key is pattern recognition — not radiology training, but clinical correlation.
High-Yield Clinical Areas for Part 2
Emergency Medicine Integration
Acute presentations dominate Part 2: MI, stroke, sepsis, diabetic emergencies, respiratory failure. Master the immediate management algorithms, but understand the evidence behind each step. Why aspirin and clopidogrel together? What drives the choice between CPAP and intubation?
Chronic Disease Management
Heart failure optimization, COPD exacerbation management, diabetes control, and anticoagulation decisions require understanding both acute intervention and long-term strategy. Part 2 tests both.
Specialty Interface Conditions
Conditions requiring multidisciplinary input appear frequently: inflammatory bowel disease, connective tissue disorders, hematological malignancies, and psychiatric presentations with medical complications.
Part 2 Preparation Strategy
Mechanism-First Approach
Build on your Part 1 knowledge. When you study heart failure management, connect the pathophysiology (reduced ejection fraction, neurohormonal activation) to the therapeutic ladder (ACE inhibitors, beta-blockers, MRAs). When learning renal tubular acidosis, understand both the biochemical derangement and clinical presentation.
For complex pathophysiological concepts that require deeper understanding, Rezzy AI tutor can provide conversational explanations that connect mechanisms to clinical presentations — exactly what Part 2 demands.
Case-Based Learning
Replace passive reading with active case analysis. For every condition, work through: How does it present? What investigations confirm the diagnosis? What immediate and long-term management is required? What complications should I monitor for?
Statistics Integration
Dont treat biostatistics as separate from clinical medicine. When studying trial data for cardiac interventions, understand the NNT for statins in primary prevention, the bleeding risk with dual antiplatelet therapy, and how to counsel patients using absolute risk reduction.
PACES Preparation: From Knowledge to Clinical Competence
PACES isnt an OSCE — its a clinical competency assessment. The examiners dont want regurgitated knowledge; they want to see you function as a clinician. Success requires demonstrating clinical reasoning, communication skills, and professionalism under observation.
Station-by-Station Strategy
Stations 1 & 4: Communication Skills
These stations test your ability to explain complex medical information, obtain informed consent, and handle difficult conversations. Success requires structure, empathy, and clear language.
Common scenarios include explaining new diagnoses (heart failure, diabetes), discussing treatment options (anticoagulation risks and benefits), and addressing patient concerns. The key is adapting your explanation to the patient's educational level and emotional state.
Practice with Clinical Rounds simulations to develop natural conversation flow and receive feedback on your communication approach before facing real examiners.
Stations 2 & 5: Clinical Consultations
These 20-minute stations combine history-taking, focused examination, and clinical reasoning. You have 15 minutes with the patient, then 5 minutes explaining your findings and differential diagnosis to examiners.
Structure is essential:
1. History (8-10 minutes): Presenting complaint, history of presenting complaint, systems review targeting your differential, relevant past history, drug history, social history
2. Examination (5-7 minutes): Focused examination based on your clinical suspicions
3. Examiner Discussion (5 minutes): Present findings, offer differential diagnosis, suggest investigations and management
Station 3: Cardiovascular & Neurological Examination
These focused examinations test your technical skills and ability to elicit physical signs. For cardiology, master heart sounds, murmur characterization, and signs of heart failure. For neurology, develop systematic approaches to motor, sensory, and coordination examination.
The cardiovascular system connects directly to your Part 1 physiology knowledge — when you find a displaced apex beat with third heart sound, connect this to elevated left ventricular end-diastolic pressure and heart failure pathophysiology.
Clinical Examination Techniques
Cardiovascular System
Master the sequence: inspection, palpation, auscultation. Look for peripheral signs (clubbing, cyanosis, peripheral edema), assess pulse character and blood pressure, then systematic cardiac auscultation. Know how to position patients for optimal murmur detection.
Respiratory System
Inspection for chest wall movement asymmetry, percussion for effusions and consolidation, auscultation for wheeze, crackles, and reduced air entry. Connect examination findings to underlying pathophysiology.
Abdominal System
Systematic approach prevents missing key findings. Inspection, light and deep palpation, percussion for organomegaly and shifting dullness, auscultation for bowel sounds. Know how to examine for ascites and hepatosplenomegaly.
Neurological System
Upper limb, lower limb, and cranial nerve examinations require smooth technique and accurate interpretation. Master power assessment, reflex testing, and coordination examination. Connect anatomical findings to functional deficits.
PACES Success Principles
Clinical Reasoning Over Pattern Recognition
PACES rewards candidates who demonstrate thinking, not just observation. When you find a systolic murmur, dont just identify it — explain its characteristics, what they suggest about the underlying pathology, and what further assessment you would perform.
Professional Communication
Address patients by name, maintain eye contact, explain what you're doing during examination. Thank patients and ensure their comfort. These seemingly minor points significantly influence examiner scoring.
Structured Presentation
When discussing cases with examiners, use clear structure: "This 67-year-old gentleman presents with... On examination, I found... This suggests... I would like to investigate with... and my management would include..."
Integration Strategy: One Exam, Not Three
The candidates who excel at MRCP treat it as one continuous learning journey, not three separate mountains to climb. Here's how to build that integrated approach:
Knowledge Layering System
Layer 1: Mechanisms (Part 1 Focus)
Build your foundation with pathophysiology and pharmacology. But dont study these in isolation — always connect to clinical presentations you might encounter in later stages.
Layer 2: Application (Part 2 Focus)
Take your mechanistic understanding and apply it to clinical vignettes. When studying heart failure, progress from pathophysiology to diagnostic criteria to treatment algorithms to prognostic factors.
Layer 3: Practice (PACES Focus)
Transform your clinical knowledge into practical skills. Practice explaining heart failure pathophysiology to patients in lay terms. Develop smooth examination techniques that efficiently elicit the signs you've studied.
Revision Cycles
Daily Integration (Throughout Preparation)
Spend 30 minutes daily connecting your current focus area across all three exam levels. If studying cardiology for Part 1, spend time on Part 2 cardiology vignettes and practice cardiovascular examination technique.
Weekly Cross-Linking (Every Weekend)
Review the previous week's content from an integrated perspective. How does the pharmacology you studied connect to clinical decision-making? How do the examination techniques relate to underlying pathophysiology?
Monthly Consolidation (End of Each Month)
Full integration review. Take a complex case — say, a patient with heart failure and atrial fibrillation — and work through it from Part 1 mechanisms through Part 2 management decisions to PACES consultation skills.
Common Preparation Mistakes to Avoid
Most MRCP candidates make predictable errors that derail their preparation. Avoid these pitfalls:
Treating PACES as an OSCE
PACES tests clinical competence, not performance. Examiners want to see you think like a doctor, not recite examination sequences. Focus on clinical reasoning and professional communication, not just technical accuracy.
Memorizing Without Understanding
Part 2 questions often test principles, not facts. Understanding why beta-blockers improve heart failure outcomes matters more than memorizing the specific drugs. When mechanisms make sense, applications become obvious.
Isolating Each Stage
The biggest mistake is preparing for each component independently. Part 1 biochemistry directly informs Part 2 metabolic emergencies. Part 2 clinical reasoning feeds into PACES consultation discussions.
Underestimating Time Management
Each component requires different time management strategies. Part 1 and 2 demand rapid question processing — about 1.8 minutes per question. PACES requires balancing thoroughness with efficiency across 20-minute stations.
Neglecting Communication Practice
Many clinically excellent candidates fail PACES on communication skills. Practice explaining complex medical concepts in simple language. Record yourself taking histories and presenting cases.
Creating Your 2026 Study Timeline
An effective MRCP preparation requires strategic timing and realistic goal-setting. Here's a framework adaptable to your circumstances:
6-Month Intensive Plan
Months 1-2: Part 1 Foundation
Week 1-2: Cardiovascular and respiratory physiology
Week 3-4: Renal and neurological systems
Week 5-6: Endocrine and hematological systems
Week 7-8: Pharmacology integration and practice questions
Months 3-4: Part 2 Clinical Development
Week 9-10: Emergency medicine and acute care
Week 11-12: Chronic disease management
Week 13-14: Evidence-based medicine and statistics
Week 15-16: Full-length mock examinations
Months 5-6: PACES Skill Development
Week 17-18: History-taking and communication skills
Week 19-20: Systematic examination techniques
Week 21-22: Clinical reasoning and case presentation
Week 23-24: Mock PACES and final integration
12-Month Extended Plan
For candidates balancing clinical work with preparation, extend the timeline:
Months 1-4: Part 1 preparation with slower pace
Months 5-8: Part 2 clinical development
Months 9-12: PACES preparation and integration
Adjust based on your baseline knowledge and clinical experience. Recent graduates may need more Part 1 foundation time, while experienced clinicians might accelerate through basic science and focus on PACES skills.
Resource Optimization
Effective preparation requires selecting resources that support integration rather than compartmentalization:
Question Banks
Choose platforms offering detailed explanations that connect basic science to clinical applications. Look for questions that mirror exam format and difficulty.
Textbooks and References
Oxford Handbook of Clinical Medicine: Practical clinical management
Kumar & Clark's Clinical Medicine: Comprehensive pathophysiology
Oxford Textbook of Medicine: Advanced clinical reasoning
Digital Learning Modern preparation benefits from adaptive learning platforms. Oncourse's integrated approach combines spaced repetition flashcards with AI-powered explanations, helping you build connections between basic science knowledge and clinical applications efficiently. Practice Partners
PACES preparation requires human feedback. Form study groups for history-taking practice and examination technique refinement. Schedule regular mock consultations with colleagues.
Exam Day Excellence
Success on MRCP exam days requires more than knowledge — it demands optimal performance under pressure:
Part 1 & 2 Written Strategy
Time Management
Aim for 1.5 minutes per question on first pass
Flag uncertain questions for review
Reserve 15 minutes for flagged question review
Guess intelligently — no negative marking
Question Analysis
Read the question stem completely before looking at options
Identify what clinical principle is being tested
Eliminate obviously incorrect options first
Choose the best answer from remaining options
PACES Performance
Professional Presence
Dress professionally and maintain composure
Address patients respectfully throughout
Thank patients and ensure comfort
Stay calm when facing challenging cases
Station Management
Read station instructions carefully
Manage time efficiently but dont appear rushed
Present findings clearly and systematically
Answer examiner questions directly and confidently
Frequently Asked Questions
How long should I prepare for MRCP?
Preparation time varies based on your clinical experience and baseline knowledge. Most candidates require 6-12 months of focused study. Recent graduates typically need longer for Part 1 basic science, while experienced clinicians may accelerate through foundational content but require more time developing PACES communication skills.
Can I take Part 2 before passing Part 1?
No, you must pass Part 1 before attempting Part 2 Written. However, you can take PACES after passing Part 1, even if you havent attempted Part 2 Written. Many candidates find attempting PACES after Part 1 builds clinical confidence for Part 2.
What pass rates should I expect?
Pass rates vary by component and candidate experience. Part 1 typically sees 40-50% pass rates. Part 2 Written has slightly higher pass rates around 60-70%. PACES pass rates range from 50% for candidates 2-3 years post-graduation to 77% for those 3-4 years post-graduation.
How do I know when Im ready?
Consistent mock exam scores above 65% indicate readiness for written components. For PACES, comfortable performance in mock examinations with positive feedback from multiple examiners suggests readiness. Dont postpone exams seeking perfection — competence is the standard, not excellence.
Should I use multiple question banks?
Focus on one comprehensive question bank rather than scattered resources. Depth matters more than breadth. Choose a platform with detailed explanations and track your progress systematically. Multiple superficial resources often create confusion rather than clarity.
How important are examination techniques for PACES?
Technical examination skills are important but secondary to clinical reasoning and communication. Examiners prefer candidates who demonstrate clear thinking and professional interaction over those with perfect technique but poor reasoning. Master basic techniques thoroughly, then focus on clinical interpretation and patient communication.
Your Next Steps
MRCP preparation succeeds when you treat it as integrated clinical development, not three separate examinations. Start with a clear timeline, choose quality resources that support knowledge integration, and practice regularly with feedback.
Build your foundation with solid basic science understanding, develop clinical reasoning through case-based learning, and refine practical skills through deliberate practice. Most importantly, maintain perspective — MRCP tests clinical competence, not perfection.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for MRCP success. Download free on Android and iOS.