Back
High-Yield NEET Questions: Bronchogenic Carcinoma X-ray & CT Findings 2026
Master bronchogenic carcinoma imaging for NEET-PG 2026. Complete guide to X-ray and CT findings, staging criteria, and high-yield question patterns with expert insights.
High-Yield NEET Questions: Bronchogenic Carcinoma X-ray & CT Findings 2026
Bronchogenic carcinoma remains one of the most frequently tested topics in NEET-PG radiology sections, with imaging findings being a cornerstone of diagnosis and staging. Every year, 8-12% of radiology questions in NEET-PG focus on lung pathology, making bronchogenic carcinoma X-ray and CT findings absolutely essential for exam success.
Understanding the radiological patterns of different histological types, their typical locations, and associated complications can easily secure 15-20 marks in your NEET-PG exam. This comprehensive guide covers all high-yield imaging findings that repeatedly appear in NEET-PG questions, complete with must-know facts and clinical correlations.
Understanding Bronchogenic Carcinoma: The NEET-PG Perspective
Bronchogenic carcinoma accounts for approximately 85-90% of all lung cancers, making it the most important lung malignancy from an exam standpoint. The term "bronchogenic" indicates origin from the bronchial epithelium, though modern understanding shows these tumors can arise from various parts of the respiratory tree.
Key Classification for NEET-PG
Primary Categories:
Non-Small Cell Lung Cancer (NSCLC) - 85% of cases
- Squamous cell carcinoma (25-30%)
- Adenocarcinoma (40-45%)
- Large cell carcinoma (5-10%)
Small Cell Lung Cancer (SCLC) - 15% of cases
This classification is crucial because each type has distinct imaging characteristics, preferred locations, and growth patterns that are heavily tested in NEET-PG.
High-Yield Location Patterns
Histological Type | Preferred Location | Key Imaging Feature |
|---|---|---|
Squamous Cell Carcinoma | Central/hilar | Cavitation common |
Adenocarcinoma | Peripheral | Ground-glass opacity |
Small Cell Carcinoma | Central/mediastinal | Extensive lymphadenopathy |
Large Cell Carcinoma | Peripheral | Large, irregular mass |
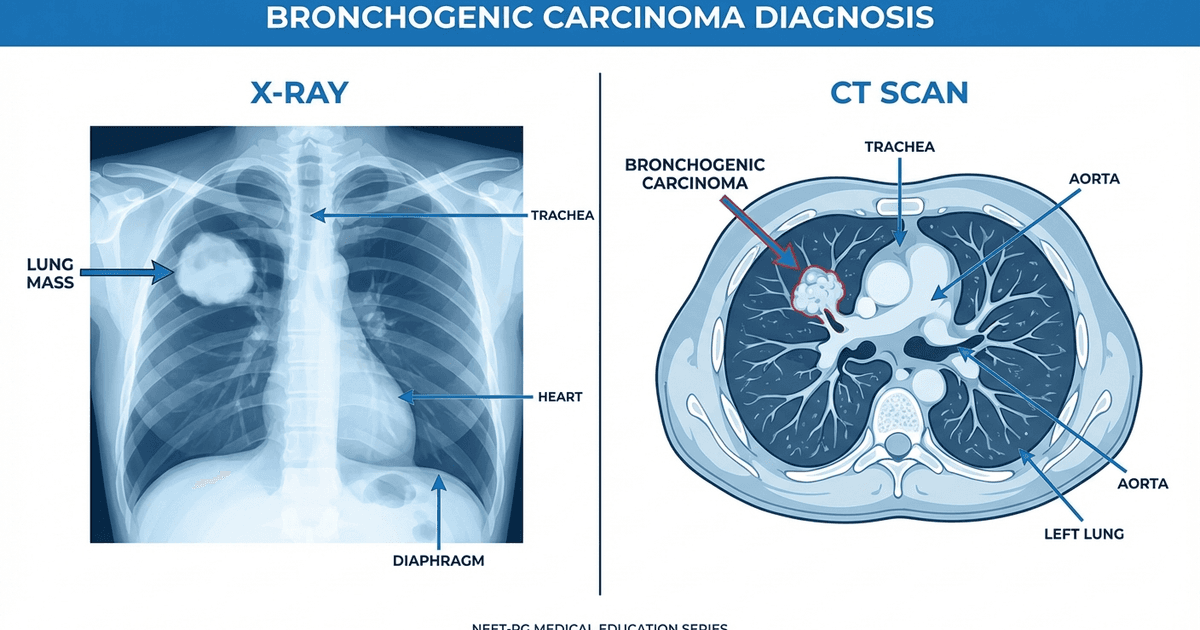
Chest X-ray Findings: High-Yield NEET Points
Primary Mass Characteristics
1. Central Masses (Squamous Cell & SCLC)
Location: Perihilar region, often obscuring normal hilar structures
Appearance: Irregular, spiculated margins
Size: Variable, but often large at presentation
Associated findings: Hilar lymphadenopathy, post-obstructive pneumonia
Key NEET Fact: Central masses causing bronchial obstruction lead to the "S sign of Golden" - a reverse-S shaped opacity combining the mass with adjacent atelectasis. 2. Peripheral Masses (Adenocarcinoma & Large Cell)
Location: Outer third of lung fields
Appearance: Round to oval masses with irregular borders
Size: Often smaller at detection (screening programs)
Associated findings: Pleural retraction, chest wall invasion
High-Yield Point: Peripheral adenocarcinomas may present as ground-glass nodules (GGNs) on CT, representing lepidic growth pattern.
Cavitation Patterns - Exam Favorite
Cavitation is one of the most tested features in NEET-PG bronchogenic carcinoma questions:
Squamous Cell Carcinoma:
Most likely to cavitate (30-60% of cases)
Thick-walled cavities with irregular inner margins
"Shaggy" or nodular cavity walls
Adenocarcinoma:
Rarely cavitates (5-10% of cases)
When present, usually thin-walled
Small Cell Carcinoma:
Almost never cavitates
If cavitation seen, question the diagnosis
Secondary Signs on Chest X-ray
1. Atelectasis/Collapse
Segmental or lobar collapse
Volume loss with mediastinal shift
Compensatory hyperinflation of remaining lung
2. Post-obstructive Pneumonia
Recurrent infections in same location
"Golden pneumonia" sign in elderly patients
Delayed resolution despite appropriate antibiotics
3. Pleural Effusion
Unilateral in 50% of cases at presentation
May be malignant (exudative) or reactive
Massive effusion suggests pleural metastases
CT Scan Findings: Advanced Imaging Insights
High-Resolution CT Characteristics
1. Nodule Morphology
Spiculation: Radiating linear strands from nodule margin
Ground-glass appearance: Increased attenuation with visible vessels
Solid components: Within ground-glass lesions (mixed density)
2. Enhancement Patterns
Arterial phase: Early enhancement >20 HU suggests malignancy
Venous phase: Continued enhancement indicates neoplasm
Delayed phase: Washout patterns help differentiate types
Location-Specific CT Findings
Upper Lobe Predilection (Squamous & Adenocarcinoma):
Right upper lobe most common overall
Apical segments frequently involved
Association with smoking history
Lower Lobe Involvement (Adenocarcinoma):
Peripheral subpleural location
Multiple small nodules (lepidic spread)
"Crazy-paving" pattern in advanced cases
Mediastinal Assessment
Lymph Node Staging (Crucial for NEET-PG):
Station | Location | Size Criteria | Clinical Significance |
|---|---|---|---|
2R/2L | Upper paratracheal | >10mm short axis | N2 disease |
4R/4L | Lower paratracheal | >10mm short axis | Resectability assessment |
5 | Aortopulmonary | >10mm short axis | N2 disease |
7 | Subcarinal | >10mm short axis | Poor prognosis |
10R/10L | Hilar | >10mm short axis | N1 disease |
High-Yield NEET Fact: Subcarinal lymph node involvement (Station 7) is considered N2 disease regardless of primary tumor location.
Advanced CT Features and Complications
Vascular Invasion Assessment
Pulmonary Vessel Encasement:
>90° circumferential contact suggests invasion
Narrowing or occlusion of pulmonary arteries
Collateral circulation development
Superior Vena Cava (SVC) Syndrome:
Compression or invasion of SVC
Collateral venous drainage
Most common with right upper lobe tumors
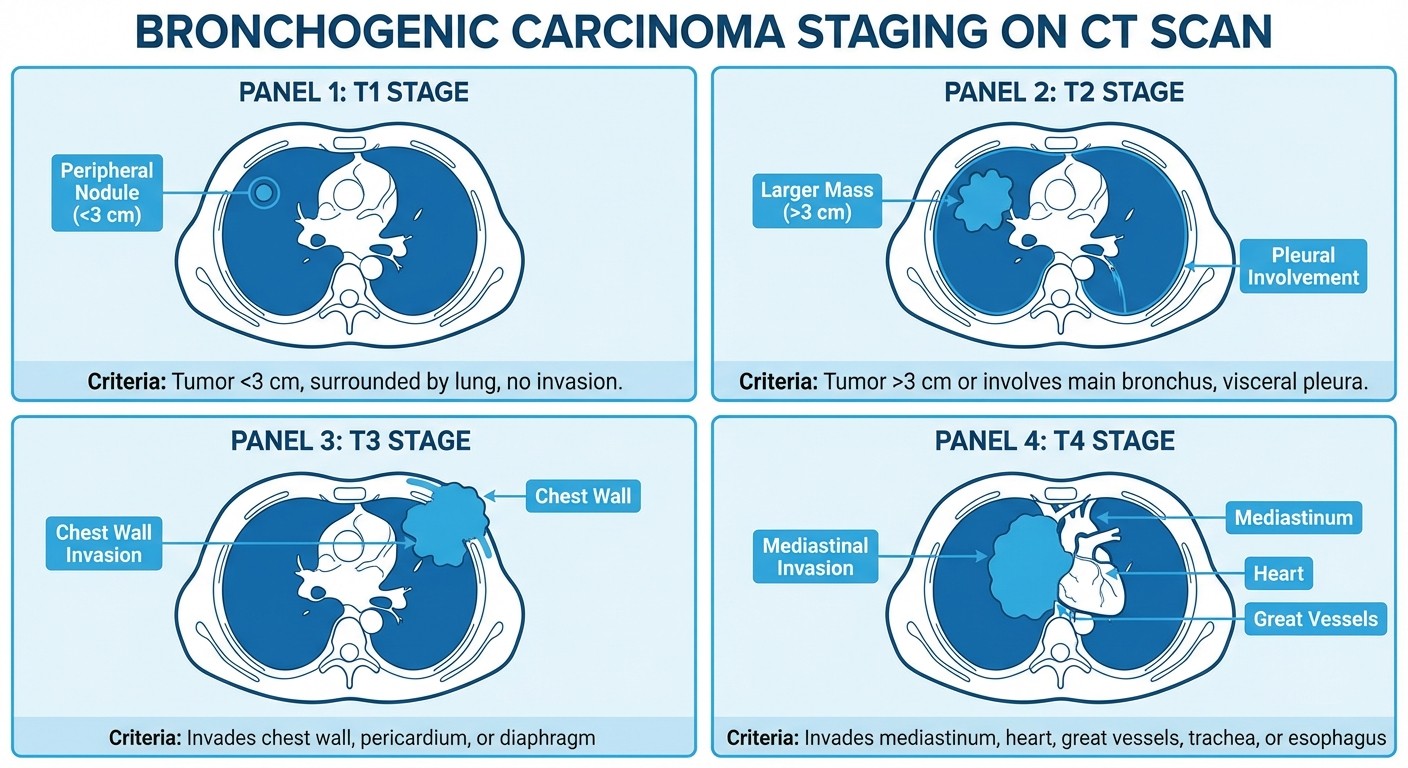
Chest Wall and Mediastinal Invasion
T3/T4 Assessment Criteria:
T3: Chest wall invasion, phrenic nerve involvement
T4: Mediastinal structure invasion (heart, great vessels, trachea)
Pancoast tumors: Apical tumors with rib destruction, brachial plexus involvement
Differential Diagnosis: High-Yield Distinguishing Features
Benign vs Malignant Characteristics
Favoring Malignancy:
Spiculated margins
Rapid growth (doubling time <400 days)
Size >2cm
Eccentric calcification
Enhancement >20 HU
Favoring Benign Process:
Smooth, well-defined margins
Stable size >2 years
Central, diffuse, or popcorn calcification
No enhancement (<10 HU)
Common NEET-PG Differentials
1. Pulmonary Metastases
Multiple nodules
Different sizes
Peripheral distribution
Known primary malignancy
2. Inflammatory Conditions
Tuberculoma: Central calcification, satellite lesions
Pneumonia: Air bronchograms, rapid resolution
Granulomas: Slow growth, central calcification
High-Yield NEET Questions and Patterns
Frequently Tested Scenarios
Scenario 1: 60-year-old smoker with central mass and cavitation
Answer: Squamous cell carcinoma
Key: Central location + cavitation + smoking history
Scenario 2: Young female non-smoker with peripheral ground-glass nodule
Answer: Adenocarcinoma (in-situ or minimally invasive)
Key: Demographics + location + appearance
Scenario 3: Patient with recurrent pneumonia in same location
Answer: Post-obstructive pneumonia secondary to bronchogenic carcinoma
Key: Recurrent pattern + lack of resolution
Must-Know Statistics for NEET-PG
5-year survival: Stage IA (90%), Stage IV (<5%)
Smoking association: 85-90% of cases
Male:Female ratio: 2:1 (decreasing due to increased female smoking)
Peak age: 65-75 years
Screening criteria: Age 50-80, ≥20 pack-years, current smoker or quit <15 years
Staging and Prognosis: TNM Classification
T-Stage Definitions (8th Edition)
Stage | Size/Invasion Criteria |
|---|---|
T1a | ≤1cm, no invasion |
T1b | >1-2cm, no invasion |
T1c | >2-3cm, no invasion |
T2a | >3-4cm or limited invasion |
T2b | >4-5cm or limited invasion |
T3 | >5-7cm or local invasion |
T4 | >7cm or extensive invasion |
N-Stage Assessment
N1: Ipsilateral hilar/intrapulmonary nodes N2: Ipsilateral mediastinal nodes N3: Contralateral mediastinal or supraclavicular nodes
M-Stage Evaluation
M0: No distant metastases M1a: Separate tumor nodules or pleural/pericardial effusion M1b: Single extrathoracic metastasis M1c: Multiple extrathoracic metastases
Modern Imaging Advances
Low-Dose CT Screening
National Lung Screening Trial (NLST) Criteria:
Age 50-80 years
≥20 pack-year smoking history
Current smoker or quit within 15 years
Annual screening reduces mortality by 20%
PET-CT Integration
SUV (Standardized Uptake Value) Significance:
SUV <2.5: Likely benign
SUV 2.5-4.0: Indeterminate
SUV >4.0: Suspicious for malignancy
Dual-time Point Imaging:
Malignant lesions show increased uptake on delayed images
Inflammatory lesions show decreased uptake on delayed images
Complications and Associated Findings
Paraneoplastic Syndromes
SCLC Associations:
SIADH (hyponatremia)
Cushing's syndrome (ACTH production)
Lambert-Eaton myasthenic syndrome
Squamous Cell Associations:
Hypercalcemia (PTH-related protein)
Hypertrophic pulmonary osteoarthropathy
Metastatic Patterns
Common Sites: 1. Brain (25-30% of cases) 2. Bone (20-25% of cases) 3. Liver (15-20% of cases) 4. Adrenal glands (10-15% of cases)
Practice Integration with Oncourse
To master bronchogenic carcinoma imaging for NEET-PG, you need comprehensive practice with high-quality questions and detailed explanations. Oncourse's lung cancer approach lessons provide in-depth coverage of all imaging aspects, from basic X-ray interpretation to advanced CT staging.
The platform's chest radiology lessons cover radiographic signs essential for identifying bronchogenic carcinoma, while the practice questions help you apply this knowledge in exam-style scenarios.
For active recall and long-term retention, Oncourse's flashcards on lung cancer use spaced repetition to ensure you remember critical imaging findings and their clinical correlations.
Study Strategy for NEET-PG Success
High-Yield Focus Areas
1. Master the 4 main types and their typical locations
2. Understand cavitation patterns - heavily tested
3. Learn TNM staging criteria - especially T and N stages
4. Practice differential diagnosis - malignant vs benign features
5. Know complications - paraneoplastic syndromes, metastatic patterns
Common Pitfalls to Avoid
Don't assume all central masses are squamous cell carcinoma
Small cell carcinoma rarely cavitates - if you see cavitation, think squamous
Adenocarcinoma can present as ground-glass opacity, not just solid masses
Always look for mediastinal lymphadenopathy in staging questions
Quick Revision Points
Remember the "CAVES" mnemonic for high-yield features:
Cavitation (squamous cell)
Adenocarcinoma (peripheral, GGOs)
Vascular invasion (T4 staging)
Effusion (staging implications)
Small cell (central, no cavitation)
Conclusion
Bronchogenic carcinoma imaging represents a high-yield topic that can significantly impact your NEET-PG score. Focus on understanding the relationship between histological types, their preferred locations, and characteristic imaging findings. Regular practice with Oncourse's comprehensive radiology modules will help you develop the pattern recognition skills essential for exam success.
Remember that consistent practice with varied question formats and detailed case discussions will build the confidence needed to tackle any bronchogenic carcinoma question in NEET-PG 2026. Master these imaging findings, understand their clinical correlations, and you'll be well-prepared to excel in this crucial examination topic.
Ready to test your knowledge? Start practicing with Oncourse's lung cancer questions and track your progress as you build expertise in bronchogenic carcinoma imaging interpretation.