
Lung Cancer Approach — MCQs

A 45-year-old male reports several years of asbestos exposure while working in the construction industry. He reports smoking 2 packs of cigarettes per day for over 20 years. Smoking and asbestos exposure increase the incidence of which of the following diseases?
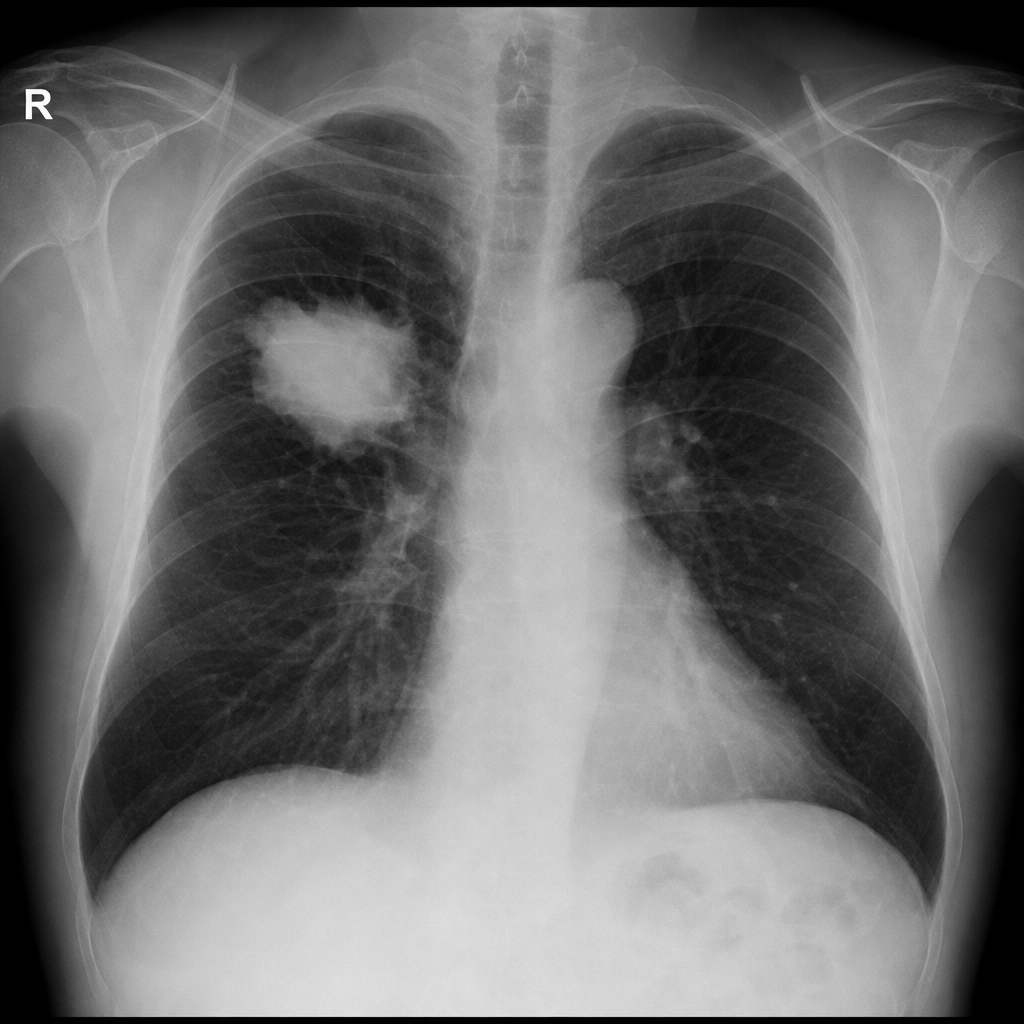
A 70-year-old smoker presents with dyspnea and weight loss. CXR shows a mass in the right lung. What is the next step?
What finding during surgery can change the staging of a tumor from Stage I to Stage II in a patient with a history of lung cancer?
Which type of lung cancer is most commonly found in non-smokers?
What is the most appropriate next step in management for a patient with a Stage III ovarian cancer with partial response to platinum-based chemotherapy?
Which of the following is the MOST characteristic feature of Eaton-Lambert syndrome?
Which of the following is a characteristic of bronchoalveolar carcinoma?
Most common symptom of lung carcinoma is
Stereotactic Radiotherapy is used in:
A 45-year-old man presents with a dry cough, fatigue, and bilateral hilar lymphadenopathy on chest X-ray. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app