FMGE Surgery High Yield Topics 2026: Complete Guide for Foreign Medical Graduates
Master FMGE surgery with this comprehensive guide covering high-yield topics, weightage breakdown, and proven study strategies for foreign medical graduates in 2026.
FMGE Surgery High Yield Topics 2026: Complete Guide for Foreign Medical Graduates
You are probably staring at your surgery textbook right now, wondering how to tackle 800+ pages for an exam that gives you 63 seconds per question. Surgery accounts for 5-8% of FMGE questions — roughly 8-13 MCQs out of 165 total. That might seem manageable, but here's the reality: surgery has one of the highest fail rates among FMGs, not because the concepts are harder, but because most students prepare wrong.
Foreign medical graduates often approach surgery like they did in medical school — reading everything, memorizing procedures they'll never perform. Wrong strategy. The FMGE tests pattern recognition, not surgical technique. You need to know hernias well enough to spot the complications in 30 seconds, not perform a laparoscopic repair.
This guide breaks down exactly what works: the 15 high-yield surgery topics that generate 70% of FMGE surgery questions, how to study them using active recall instead of passive reading, and the MCQ patterns that trip up even strong students.
Why Surgery Trips Up Foreign Medical Graduates
Surgery consistently ranks among the most challenging subjects for FMGs in licensing exams. Three specific factors make it brutal:
Pattern Recognition Speed: Unlike medicine where you can reason through pathophysiology, surgery questions test instant recognition. See "pain migration from umbilicus to RIF" — you should immediately think appendicitis without working through differential diagnoses. Procedure vs Concept Confusion: Most FMGs studied surgery with heavy emphasis on surgical techniques and operative procedures. FMGE surgery questions focus on indications, contraindications, complications, and anatomy — not how to actually operate. High-Stakes Anatomy: Surgery MCQs love testing surgical anatomy that you probably skimmed in medical school. Questions about fascial layers, nerve courses, and anatomical landmarks appear frequently and have zero room for approximation.
The good news? Surgery topics are finite and predictable. Master these 15 areas, and you'll handle 70-80% of surgery questions confidently.
Complete High-Yield Surgery Topics for FMGE 2026
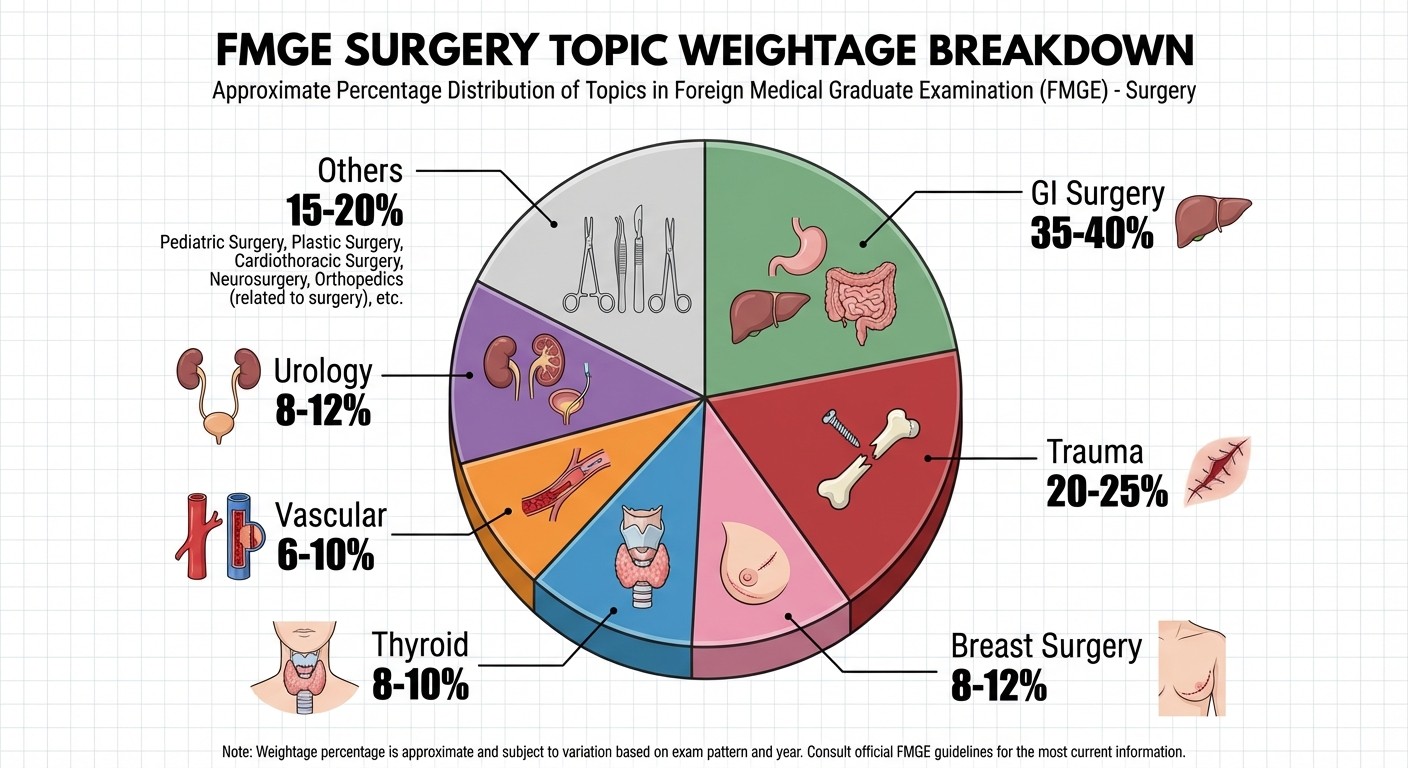
Gastrointestinal Surgery (35-40% of Surgery Questions)
Appendicitis: Classic presentation, atypical presentations in elderly/pregnant patients, McBurney's point, complications (perforation, abscess formation). Focus on Alvarado score and when to operate vs observe. Hernias: Inguinal (direct vs indirect), femoral, umbilical, incisional. Know the anatomical boundaries of Hesselbach's triangle. Practice with GI surgery MCQs to master hernia differentials. Bowel Obstruction: Small bowel vs large bowel obstruction, paralytic ileus vs mechanical obstruction. X-ray findings are frequently tested. Adhesions remain the commonest cause of SBO. Peptic Ulcer Disease: Complications requiring surgery — perforation, bleeding, outlet obstruction. Know when medical management fails and surgery becomes necessary. Gallbladder Disease: Cholecystitis vs cholelithiasis, Murphy's sign, Courvoisier's law. Laparoscopic cholecystectomy contraindications appear regularly.
Using Oncourse's smart question bank with surgery filters helps you drill these GI topics systematically instead of random grinding across all surgical subspecialties.
Trauma Surgery (20-25% of Surgery Questions)
ATLS Principles: Primary survey (ABCDE), secondary survey, Glasgow Coma Scale. Trauma questions follow ATLS algorithms religiously. Head Trauma: Extradural vs subdural vs subarachnoid hemorrhage. CT findings, indications for immediate surgery, ICP management. Chest Trauma: Pneumothorax (tension vs simple), hemothorax, flail chest, cardiac tamponade. Know when to do needle decompression vs chest tube. Abdominal Trauma: Blunt vs penetrating, FAST scan, diagnostic peritoneal lavage indications. Spleen and liver injuries dominate questions. Fractures: Open vs closed fractures, compartment syndrome, fat embolism syndrome. Orthopedic emergencies that need immediate intervention. Master trauma surgery concepts with systematic approach to injury assessment and management priorities.
Breast Surgery (8-12% of Surgery Questions)
Breast Cancer: TNM staging, hormone receptor status, surgical options (lumpectomy vs mastectomy). Know indications for each approach. Benign Breast Disease: Fibroadenoma vs phyllodes tumor vs fibrocystic disease. Age-based approach to breast lumps. Inflammatory Conditions: Mastitis vs breast abscess, lactational vs non-lactational abscess management.
Thyroid and Parathyroid Surgery (8-10% of Surgery Questions)
Thyroid Nodules: Fine needle aspiration indications, bethesda classification, cold vs hot nodules on scintigraphy. Thyroid Cancer: Papillary vs follicular vs medullary vs anaplastic. Surgical extent based on histology. Hyperthyroidism: Medical vs surgical management, indications for thyroidectomy in Graves' disease. Parathyroid Disease: Primary vs secondary vs tertiary hyperparathyroidism, indications for parathyroidectomy.
Vascular Surgery (6-10% of Surgery Questions)
Peripheral Arterial Disease: Claudication vs rest pain vs gangrene, ankle-brachial index, revascularization options. Venous Disease: Varicose veins, deep vein thrombosis, chronic venous insufficiency. Aneurysms: Abdominal aortic aneurysm screening, rupture vs expansion, surgical thresholds. Review vascular trauma patterns that combine trauma and vascular surgery concepts.
Urology Basics (8-12% of Surgery Questions)
Urolithiasis: Calcium vs uric acid vs struvite stones, medical vs surgical management, ESWL indications. Benign Prostatic Hyperplasia: Medical management failure, surgical options (TURP vs open prostatectomy). Urological Emergencies: Testicular torsion vs epididymitis, paraphimosis, acute urinary retention. Genitourinary Trauma: Kidney, ureter, bladder, urethral injuries. Practice urological trauma scenarios for pattern recognition.
Wounds and Healing (5-8% of Surgery Questions)
Wound Classification: Clean, clean-contaminated, contaminated, dirty wounds. Antibiotic prophylaxis protocols follow WHO surgical safety guidelines. Wound Healing: Primary vs secondary intention, factors affecting healing, keloid vs hypertrophic scars. Surgical Site Infections: Risk factors, prevention, management. CDC classification system.
Surgical Anatomy Essentials (10-15% of Surgery Questions)
Inguinal Canal: Layers, boundaries, contents. Differentiating direct vs indirect hernias anatomically. Femoral Triangle: Boundaries, contents, relations. Femoral hernia anatomy. Hepatobiliary Anatomy: Calot's triangle, bile duct anatomy, hepatic segments. Neck Anatomy: Thyroid relations, recurrent laryngeal nerve course, parathyroid locations.
Surgery anatomy questions test precise knowledge — "approximately" doesnt work. Oncourse's spaced repetition flashcards help cement anatomical facts like Courvoisier's law and Langer's lines that you need instantly accessible during the exam.
Topic Weightage Breakdown by Sub-Specialty
Surgery Sub-specialty | Expected Questions (out of 165 total) | Key Focus Areas |
|---|---|---|
Gastrointestinal Surgery | 3-4 questions | Appendicitis, hernias, bowel obstruction |
Trauma Surgery | 2-3 questions | ATLS, head trauma, chest trauma |
Breast Surgery | 1-2 questions | Breast cancer staging, benign disease |
Thyroid/Parathyroid | 1 question | Thyroid nodules, hyperthyroidism surgery |
Vascular Surgery | 1 question | PAD, aneurysms, venous disease |
Urology | 1-2 questions | Stones, BPH, GU trauma |
Surgical Anatomy | 1-2 questions | Inguinal canal, femoral triangle |
This distribution shows why GI surgery and trauma deserve 60% of your surgery study time. You cant afford to study all subspecialties equally — that's a recipe for mediocrity across everything.
Common FMG Mistakes in Surgery Preparation
Mistake #1: Procedure-Heavy Studying
Wrong approach: Memorizing surgical steps for appendectomy, cholecystectomy, hernia repair.
Right approach: Focus on indications, contraindications, complications, and anatomy.
Mistake #2: Equal Time Distribution
Wrong approach: Spending equal time on all surgery subspecialties.
Right approach: 40% time on GI surgery, 25% on trauma, 35% on remaining topics.
Mistake #3: Passive Reading Strategy
Wrong approach: Reading surgery textbooks cover to cover, highlighting everything.
Right approach: Active recall with MCQ practice and concept testing.
Mistake #4: Ignoring Surgical Anatomy
Wrong approach: Assuming basic anatomy knowledge is sufficient.
Right approach: Drilling surgical anatomy until landmarks and relations become automatic.
Oncourse's performance analytics track your accuracy across surgery subspecialties, showing exactly where you're losing marks — turning "study more surgery" into a precise improvement plan.
Recommended Revision Strategy: Active Recall vs Passive Reading
Phase 1: Foundation Building (3-4 weeks)
Week 1-2: GI Surgery and Trauma
Study one topic daily using the 25-5 rule: 25 minutes focused study, 5-minute active recall test
Cover appendicitis, hernias, bowel obstruction from GI surgery
Master ATLS principles, head trauma, chest trauma from trauma surgery
Review GI surgery lessons for systematic concept building
Week 3-4: Remaining High-Yield Topics
Breast surgery, thyroid surgery, vascular basics, urology essentials
Continue 25-5 active recall sessions
Focus on differentiating similar conditions (direct vs indirect hernia, subdural vs extradural hematoma)
Phase 2: Pattern Recognition (2-3 weeks)
Daily MCQ Practice: 20-30 surgery MCQs daily with immediate review
Focus on question pattern recognition rather than content review
Time yourself: 60 seconds per question maximum
Note recurring themes and commonly tested variations
Weekly Mock Tests: Full-length surgery sections
Simulate actual exam conditions
Identify weak areas for targeted revision
Track improvement in speed and accuracy
Using Oncourse's filtered question bank by surgery subspecialty prevents random question grinding and ensures you're drilling exactly the weak spots your analytics reveal.
Phase 3: Rapid Revision (1 week)
High-Yield Facts Review: Quick recall of surgical anatomy, key classifications, and emergency management protocols Pattern Drills: Practice identifying question types within first 10-15 seconds of reading Speed Practice: Aim for 45-second average per surgery MCQ
How to Approach Surgery MCQs: Pattern Recognition and Elimination Strategies
Pattern Recognition Techniques
Clinical Vignette Patterns:
"Young male with RIF pain that started periumbilically" = Appendicitis until proven otherwise
"Elderly female with painless jaundice and palpable gallbladder" = Malignant biliary obstruction (Courvoisier's sign)
"Road traffic accident with altered consciousness and lucid interval" = Extradural hematoma
Anatomical Question Patterns:
Questions starting with "During surgery..." usually test surgical anatomy
"Most likely structure injured..." tests anatomical relations
"Boundaries of..." tests precise anatomical knowledge
Elimination Strategies
Rule Out Impossibles First:
Eliminate options that contradict basic physiology
Remove answers with incorrect anatomical relationships
Cross out options that violate established protocols (like ATLS)
Use Clinical Logic:
In trauma scenarios, always prioritize ABCDE approach
For surgical emergencies, life-threatening complications take precedence
When unsure between conservative vs surgical management, consider patient's overall condition
Leverage Statistical Thinking:
Most common causes appear more frequently than rare conditions
Classic presentations get tested more than atypical variants
Standard management protocols are favored over experimental approaches
The key is developing automatic pattern recognition. You should spot appendicitis, inguinal hernia, or extradural hematoma within seconds of reading the clinical vignette, not after eliminating other options.
Advanced Study Techniques for Surgery Mastery
Concept Clustering Method
Group related surgical conditions by shared characteristics:
"Emergency Surgery" Cluster: Appendicitis with complications, bowel obstruction with perforation, traumatic injuries requiring immediate intervention "Anatomy-Heavy" Cluster: Hernias, thyroid surgery, vascular access procedures "Cancer Surgery" Cluster: Breast cancer, thyroid malignancy, colorectal cancer
This clustering helps you see connections between topics and prevents isolated fact memorization.
Differential Diagnosis Trees
Create decision trees for common presentations:
Acute abdomen → Location → Associated symptoms → Most likely diagnosis
Neck mass → Age + characteristics → Thyroid vs lymph node vs other
Trauma patient → Mechanism → Primary survey findings → Management priority
Active Recall Integration
Instead of reading about appendicitis, test yourself:
"What are the classic signs of appendicitis?"
"When is conservative management appropriate?"
"What complications indicate immediate surgery?"
Answer without looking, then verify. Oncourse's spaced repetition system automates this process, resurfacing surgical facts at optimal intervals so they stick through exam day.
Surgical Anatomy Deep-Dive for FMGE Success
Surgical anatomy questions are non-negotiable in FMGE. You either know the exact boundaries of Hesselbach's triangle or you dont — theres no partial credit for "approximately correct."
Critical Anatomical Areas
Inguinal Region:
Inguinal canal boundaries: Anterior wall (aponeurosis of external oblique), posterior wall (transversalis fascia), superior wall (internal oblique and transversus abdominis), inferior wall (inguinal ligament)
Hesselbach's triangle: Bounded by rectus sheath medially, inguinal ligament inferiorly, inferior epigastric artery laterally
Direct vs indirect hernia differentiation by relation to inferior epigastric artery
Femoral Triangle:
Boundaries: Inguinal ligament (superior), adductor longus (medial), sartorius (lateral)
Contents (lateral to medial): Femoral nerve, artery, vein, lymphatics (NAVL)
Femoral hernia occurs through femoral canal, medial to femoral vein
Hepatobiliary Anatomy:
Calot's triangle: Bounded by cystic artery, common hepatic duct, and liver edge
Bile duct anatomy: Right and left hepatic ducts → common hepatic duct → CBD
Critical view of safety during cholecystectomy
Thyroid Surgical Anatomy:
Recurrent laryngeal nerve course: Right nerve loops around subclavian artery, left around aortic arch
Relations to thyroid: Nerve runs in tracheoesophageal groove
Parathyroid gland locations: Superior parathyroids more constant, inferior more variable
These anatomical facts require memorization, not understanding. Access surgical anatomy flashcards for systematic retention of these critical details.
Preparing for FMGE Surgery Section: Timeline and Resources
6-Month Preparation Timeline
Months 1-2: Foundation building across all subjects
Allocate 1 week specifically to surgery high-yield topics
Focus on understanding concepts before memorization
Review basic surgical preparation to build fundamentals
Months 3-4: Subject-wise deep dive
Dedicate 2-3 weeks exclusively to surgery
Master GI surgery and trauma topics first
Complete anatomy and wound healing topics
Months 5-6: Revision and practice
Daily surgery MCQ practice (15-20 questions)
Weekly mock tests with surgery sections
Final revision of high-yield facts and anatomy
Essential FMGE Surgery Resources
According to the National Board of Examinations, FMGE follows Indian medical education standards with international best practices.
Official Guidelines: NBE FMGE Information Bulletin for updated syllabus Question Banks: Focus on Indian pattern MCQs with detailed explanations Reference Books: Bailey & Love's Surgery, SRB's Manual of Surgery for quick revision Practice Tests: Attempt surgery sections under timed conditions
The key is active practice over passive reading. Surgery knowledge becomes automatic through repeated application, not theoretical study.
Frequently Asked Questions
How many surgery questions appear in FMGE 2026?
FMGE typically includes 8-13 surgery questions out of 165 total questions, representing 5-8% of the exam. The exact number varies by exam version, but preparing for 10 questions gives you a solid target.
Which surgery topics have highest weightage in FMGE?
Gastrointestinal surgery (appendicitis, hernias, bowel obstruction) and trauma surgery (ATLS principles, head trauma) together account for 60-65% of surgery questions. Focus 65% of your surgery study time on these two areas.
How much time should I dedicate to surgery preparation?
Surgery should get 8-10% of your total FMGE study time, proportional to its exam weightage. For a 6-month preparation timeline, dedicate 3-4 weeks specifically to surgery, with ongoing revision throughout your prep.
Should I memorize surgical procedures for FMGE?
No. FMGE tests surgical decision-making, not operative technique. Focus on indications for surgery, contraindications, complications, and surgical anatomy rather than step-by-step procedures.
How do I improve speed in surgery MCQs?
Pattern recognition is key. Practice identifying the diagnosis within the first 15-20 seconds of reading the question stem. Common presentations should trigger automatic recognition: RIF pain with migration suggests appendicitis, painless jaundice with palpable gallbladder suggests malignant obstruction.
Are international surgery guidelines relevant for FMGE?
FMGE follows standard international guidelines, especially ATLS for trauma management. American College of Surgeons ATLS protocols, WHO surgical safety guidelines, and standard classification systems (ASA, TNM staging) are directly applicable.
---
Surgery success in FMGE comes down to focused preparation on high-yield topics, active recall study methods, and pattern recognition practice. You dont need to master every surgical subspecialty — you need to nail the 15 topics that generate 70% of questions.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for FMGE success. Download free on Android and iOS.