
Gastrointestinal Surgery — MCQs

On this page
What is the most common cause of posterior duodenal ulcer bleeding name the artery involved?
In which type of constipation are stimulant laxatives contraindicated or should be avoided?
Which of the following clinical features best distinguishes mechanical small bowel obstruction from paralytic ileus?
A 55-year-old patient presents to the emergency department with abdominal pain, distension, and vomiting. Imaging confirms a diagnosis of cecal volvulus. Which of the following risk factors is responsible for 50-70% of cecal volvulus cases?
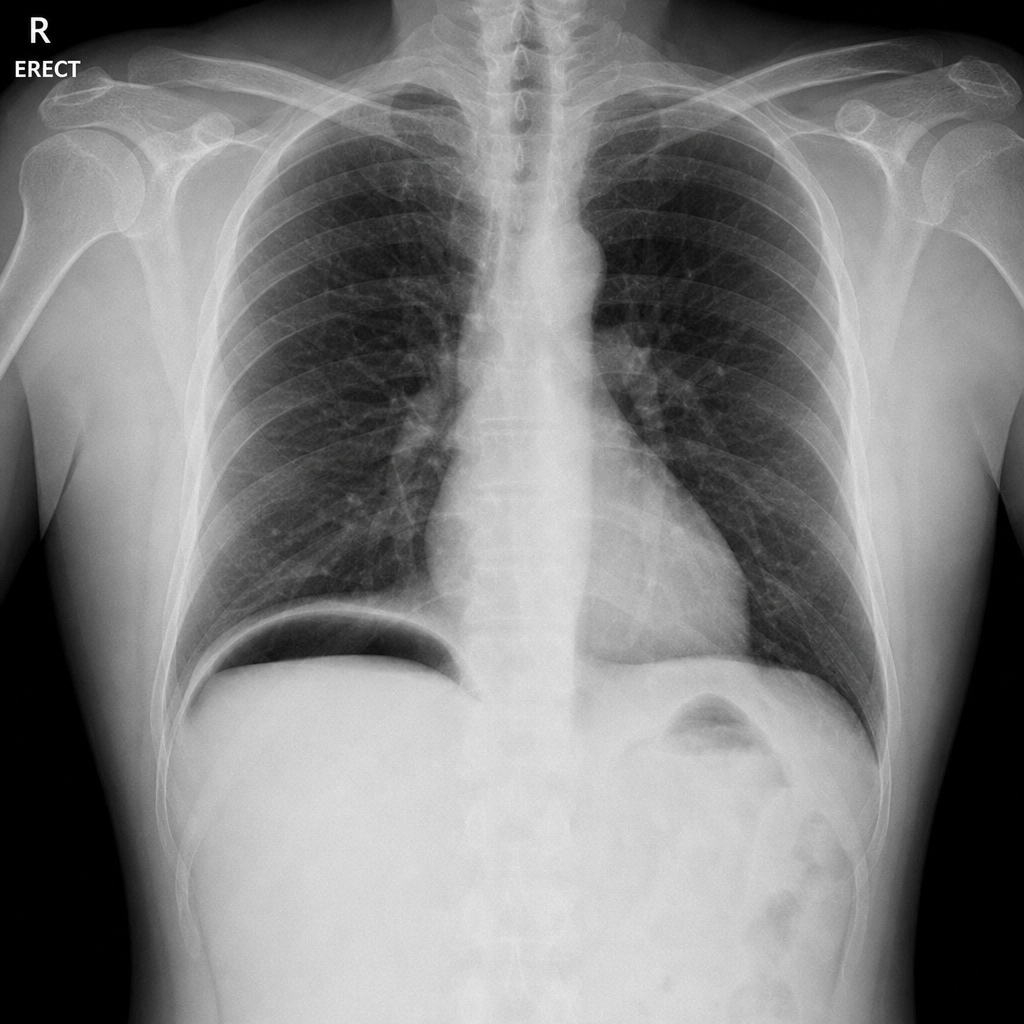
A 52-year-old male with a known history of peptic ulcer disease presents to the emergency department with sudden-onset severe epigastric pain described as 'like being stabbed', now spreading across the entire abdomen. He is lying completely still, has board-like rigidity on examination, and his vital signs show BP 118/76 mmHg, HR 92/min, RR 18/min, SpO2 98% on room air. He takes NSAIDs regularly for chronic back pain. His erect chest X-ray is shown (Image 1). After establishing IV access, sending bloods, and commencing IV fluids and analgesia, what is the most appropriate next step in management?
A 70-year-old man with atrial fibrillation presents with severe periumbilical pain out of proportion to physical findings, bloody diarrhoea, and a markedly elevated serum lactate. He is haemodynamically unstable despite initial resuscitation. A CECT abdomen is shown (Image 2). Which of the following best describes the most appropriate operative strategy for this patient?

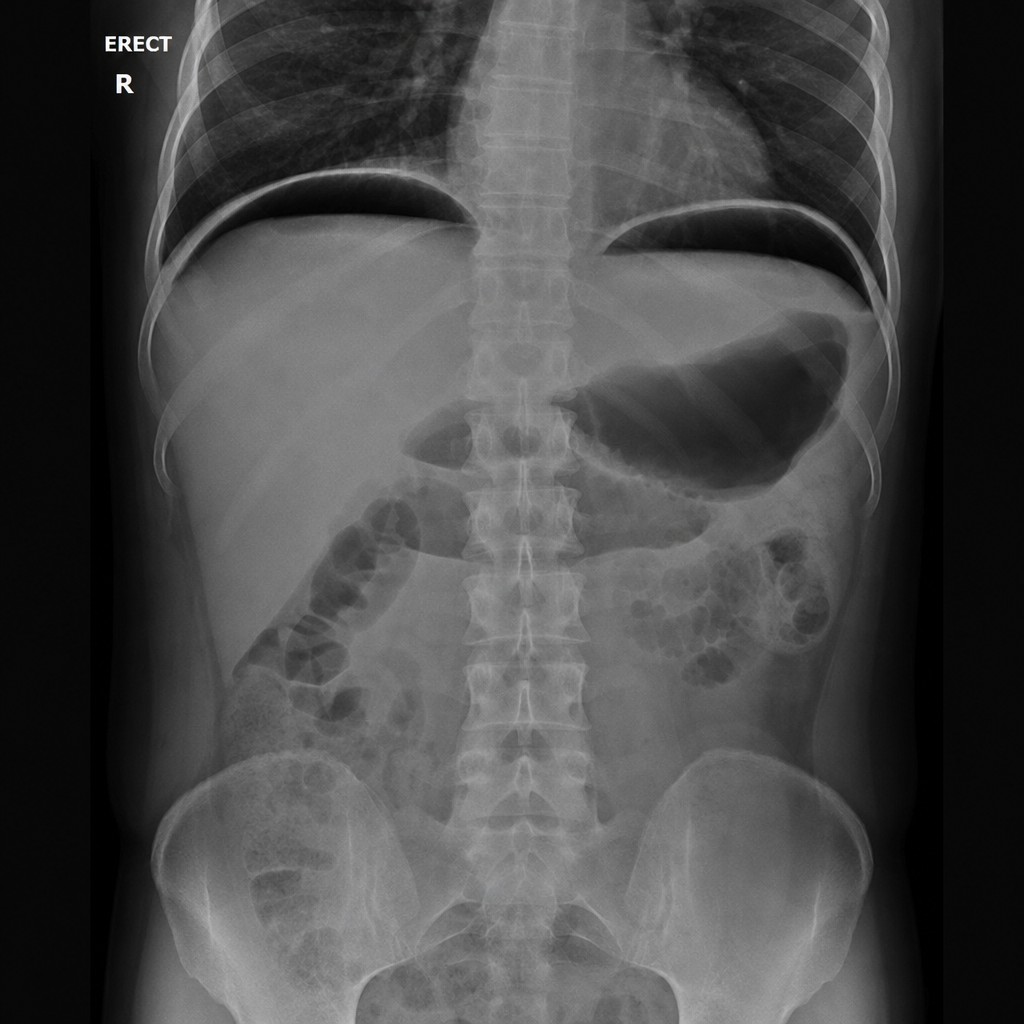
A 55-year-old man with a known history of peptic ulcer disease presents with sudden-onset severe epigastric pain that has now spread across the entire abdomen. On examination, the abdomen is board-like rigid and bowel sounds are absent. He is tachycardic and diaphoretic. His BP is 94/60 mmHg. An erect abdominal X-ray is shown (Image 1). After securing IV access and initiating fluid resuscitation, what is the most appropriate next step in management?
A 40-year-old male with a history of progressive dysphagia for liquids presents with a dilated esophagus on barium meal. What is the most likely cause?
All of the following are causes of pneumoperitoneum except?
Which of the following statements about duodenal adenocarcinoma is correct?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app