ACS US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for ACS. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
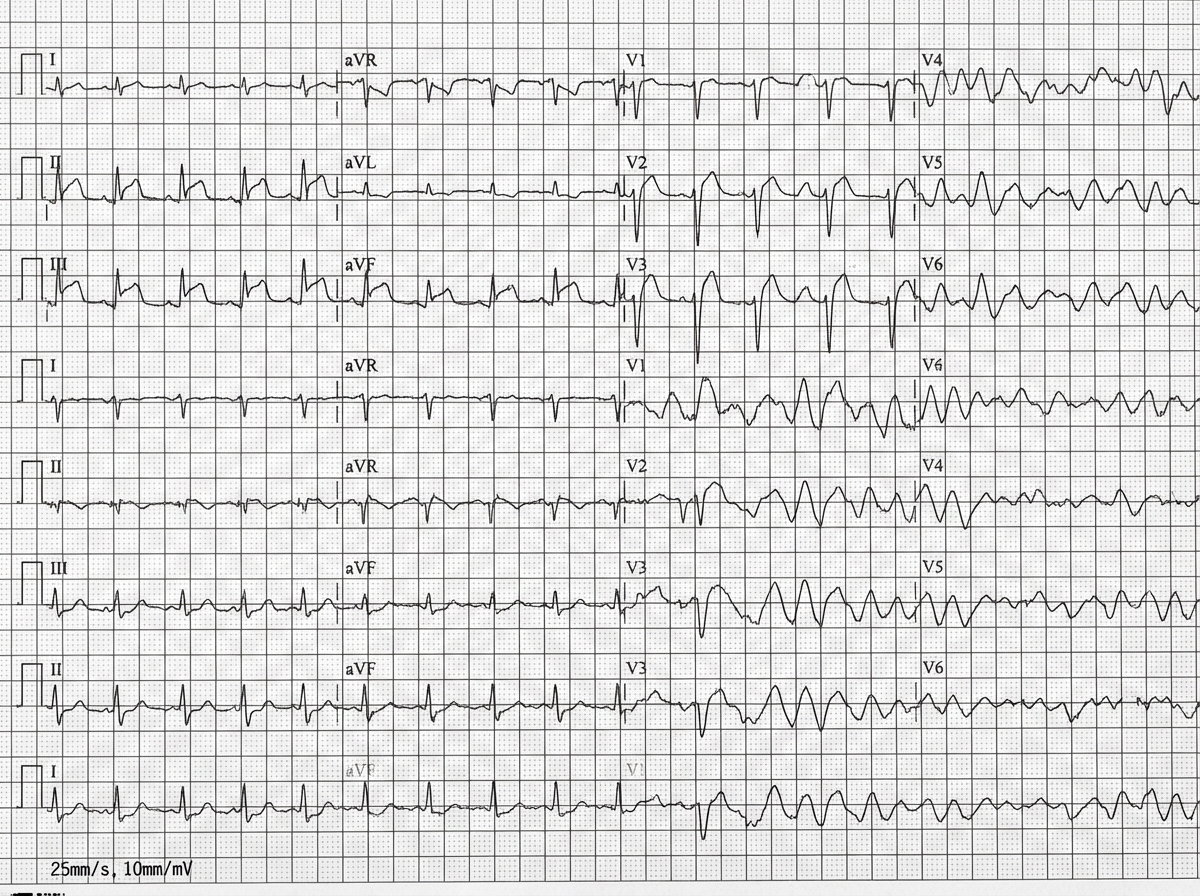
ACS US Medical PG Question 1: A 42-year-old man is brought to the emergency department 20 minutes after the sudden onset of severe chest pain, diaphoresis, shortness of breath, and palpitations. His symptoms occurred while he was at a party with friends. He has smoked one pack of cigarettes daily for 24 years. He uses cocaine occasionally. The last use was three hours ago. He appears pale. His pulse is 110/min, blood pressure is 178/106 mm Hg, and respirations are 24/min. His pupils are dilated and react sluggishly to light. The lungs are clear to auscultation. An ECG shows tachycardia and ST segment elevation in leads II, III, and aVF. While recording the ECG, the patient loses consciousness. A photo of the ECG at that point is shown. Which of the following is the most appropriate next step in management?
- A. Administer lidocaine
- B. Unsynchronized cardioversion (Correct Answer)
- C. Administer epinephrine
- D. Coronary angiography
- E. Synchronized cardioversion
ACS Explanation: ***Unsynchronized cardioversion***
- The ECG shows **ventricular fibrillation (VF)**, characterized by chaotic, irregular electrical activity without distinct QRS complexes, indicating a life-threatening arrhythmia.
- In a patient who has lost consciousness due to VF, immediate **defibrillation (unsynchronized cardioversion)** is crucial to restore normal sinus rhythm and prevent sudden cardiac death.
- Note: Unsynchronized cardioversion and defibrillation are **synonymous terms** for delivering an unsynchronized shock, with "defibrillation" being the preferred ACLS terminology for VF/pulseless VT.
*Administer lidocaine*
- While lidocaine is an **antiarrhythmic** used in some ventricular arrhythmias, it is typically administered after initial defibrillation attempts have failed or as an adjunct therapy.
- It is not the primary treatment for **unstable ventricular fibrillation**, which requires immediate electrical therapy.
*Administer epinephrine*
- Epinephrine is a **vasopressor** used during cardiac arrest to improve coronary and cerebral perfusion.
- It is administered during **cardiopulmonary resuscitation (CPR)** intervals, usually after initial defibrillation attempts, but not as the first line treatment for VF.
*Coronary angiography*
- Coronary angiography is an **invasive diagnostic procedure** to visualize coronary arteries and identify blockages, suggested by the patient's symptoms and ST elevation in the initial ECG leads.
- However, in the context of **cardiac arrest due to VF**, immediate life-saving interventions take precedence over diagnostic procedures.
*Synchronized cardioversion*
- **Synchronized cardioversion** delivers an electrical shock timed to the R-wave of the QRS complex to treat **tachyarrhythmias with a pulse** (e.g., ventricular tachycardia, atrial fibrillation with rapid ventricular response).
- It is **contraindicated in ventricular fibrillation** because there are no organized QRS complexes to synchronize with, and attempting synchronization can delay life-saving defibrillation.
ACS US Medical PG Question 2: A primary care physician who focuses on treating elderly patients is researching recommendations for secondary prevention. She is particularly interested in recommendations regarding aspirin, as she has several patients who ask her if they should take it. Of the following, which patient should be started on lifelong aspirin as monotherapy for secondary prevention of atherosclerotic cardiovascular disease?
- A. An 83-year-old female with a history of a hemorrhagic stroke 1 year ago without residual deficits
- B. A 75-year-old male who had a drug-eluting coronary stent placed 3 days ago
- C. A 67-year-old female who has diabetes mellitus and atrial fibrillation
- D. A 45-year-old female with no health problems
- E. A 63-year-old male with a history of a transient ischemic attack (Correct Answer)
ACS Explanation: **A 63-year-old male with a history of a transient ischemic attack**
- A patient with a history of **Transient Ischemic Attack (TIA)** has a high risk of subsequent stroke and should be on **lifelong aspirin monotherapy** for secondary prevention of **atherosclerotic cardiovascular disease (ASCVD)**.
- Aspirin helps prevent further thrombotic events by inhibiting platelet aggregation, making it a cornerstone for secondary prevention after TIA or ischemic stroke.
*An 83-year-old female with a history of a hemorrhagic stroke 1 year ago without residual deficits*
- Aspirin is generally **contraindicated** in patients with a history of **hemorrhagic stroke** due to the increased risk of recurrent bleeding.
- In such cases, the risks of aspirin therapy typically **outweigh the benefits** for cardiovascular prevention.
*A 75-year-old male who had a drug-eluting coronary stent placed 3 days ago*
- A patient with a recently placed **drug-eluting stent (DES)** requires **dual antiplatelet therapy (DAPT)**, typically aspirin plus a P2Y12 inhibitor, for a specific duration (e.g., 6-12 months), not aspirin monotherapy.
- Monotherapy with aspirin alone would be **insufficient** to prevent stent thrombosis in the immediate post-stenting period.
*A 67-year-old female who has diabetes mellitus and atrial fibrillation*
- This patient has two significant risk factors requiring specific management: **diabetes mellitus** for cardiovascular risk and **atrial fibrillation** for stroke risk.
- For atrial fibrillation, **anticoagulation with warfarin or a direct oral anticoagulant (DOAC)** is typically indicated, which makes aspirin monotherapy either unnecessary or potentially harmful if used alone.
*A 45-year-old female with no health problems*
- There is no indication for **aspirin primary prevention** in this patient, especially given the increased risk of bleeding without a clear cardiovascular benefit.
- Guidelines currently recommend against routine aspirin use for primary prevention in healthy individuals due to the **unfavorable risk-benefit ratio**.
ACS US Medical PG Question 3: A 71-year-old man develops worsening chest pressure while shoveling snow in the morning. He tells his wife that he has a squeezing pain that is radiating to his jaw and left arm. His wife calls for an ambulance. On the way, he received chewable aspirin and 3 doses of sublingual nitroglycerin with little relief of pain. He has borderline diabetes and essential hypertension. He has smoked 15–20 cigarettes daily for the past 37 years. His blood pressure is 172/91 mm Hg, the heart rate is 111/min and the temperature is 36.7°C (98.0°F). On physical examination in the emergency department, he looks pale, very anxious and diaphoretic. His ECG is shown in the image. Troponin levels are elevated. Which of the following is the best next step in the management of this patient condition?
- A. CT scan of the chest with contrast
- B. Echocardiography
- C. Fibrinolysis
- D. Clopidogrel, atenolol, anticoagulation and monitoring (Correct Answer)
- E. Oral nifedipine
ACS Explanation: ***Clopidogrel, atenolol, anticoagulation and monitoring***
- The ECG shows **ST depression in multiple leads (II, III, aVF, V3-V6)** and **ST elevation in aVR and V1**, which is highly suggestive of **non-ST elevation myocardial infarction (NSTEMI)** or a **posterior MI/extensive anterior ischemia**. Given the elevated troponin, the patient has an NSTEMI.
- Initial management for NSTEMI includes **dual antiplatelet therapy (aspirin and clopidogrel)**, **anticoagulation (e.g., heparin)**, and **beta-blockers (atenolol)**, along with continuous monitoring.
*CT scan of the chest with contrast*
- A CT scan with contrast would be indicated if **aortic dissection** was suspected, but the classic ECG findings and elevated troponins point away from that diagnosis as the primary concern.
- While other causes of chest pain should be considered, the **ECG and troponin elevation** make **acute coronary syndrome (ACS)** the most immediate and critical diagnosis.
*Echocardiography*
- Echocardiography is useful for assessing **cardiac function, wall motion abnormalities, and valvular disease**, but it is generally not the immediate next step in an NSTEMI after the initial stabilization and medication.
- It could be performed later to evaluate for complications such as **ventricular dysfunction** or **valvular issues**.
*Fibrinolysis*
- **Fibrinolysis** is indicated for **ST-elevation myocardial infarction (STEMI)** when PCI is not readily available, or for other thrombotic events, but not for NSTEMI.
- In NSTEMI, the primary treatment strategy includes **antiplatelets, anticoagulants**, and often **early invasive procedures (PCI)**, if indicated by risk stratification.
*Oral nifedipine*
- **Nifedipine**, a dihydropyridine calcium channel blocker, can be used for hypertension or angina, but it is **not first-line** therapy for **acute coronary syndrome**.
- **Beta-blockers like atenolol** are preferred in ACS to reduce myocardial oxygen demand and improve outcomes, whereas nifedipine can sometimes acutely worsen ischemia due to reflex tachycardia.
ACS US Medical PG Question 4: A cardiologist is studying how a new virus that infects the heart affects the electrical conduction system of the cardiac myocytes. He decides to obtain electrocardiograms on patients with this disease in order to see how the wave patterns and durations change over time. While studying these records, he asks a medical student who is working with him to interpret the traces. Specifically, he asks her to identify the part that represents initial ventricular depolarization. Which of the following characteristics is most consistent with this feature of the electrocardiogram?
- A. Elevated in patients with full thickness ischemic injury of the heart
- B. Becomes peaked in states of hyperkalemia
- C. Becomes prominent in states of hypokalemia
- D. Normal duration defined as less than 120 milliseconds (Correct Answer)
- E. Normal duration defined as less than 200 milliseconds
ACS Explanation: ***Normal duration defined as less than 120 milliseconds***
- The question asks for the representation of **initial ventricular depolarization**, which corresponds to the **QRS complex** on an ECG.
- The normal duration of the **QRS complex** is typically less than **0.12 seconds (120 milliseconds)**, reflecting efficient ventricular depolarization.
*Elevated in patients with full thickness ischemic injury of the heart*
- This description refers to the **ST segment elevation** seen in **ST-segment elevation myocardial infarction (STEMI)**, which represents myocardial injury, not initial ventricular depolarization.
- While related to cardiac electrical activity, **ST segment elevation** is a consequence of injury and refers to repolarization abnormalities, not the QRS complex itself.
*Becomes peaked in states of hyperkalemia*
- **Peaked T waves** are characteristic of **hyperkalemia**, indicating altered ventricular repolarization, not ventricular depolarization.
- The T wave represents ventricular repolarization, and its morphology changes significantly with potassium imbalances.
*Becomes prominent in states of hypokalemia*
- A **prominent U wave** is sometimes observed in **hypokalemia**, which follows the T wave and is thought to represent repolarization of Purkinje fibers.
- The U wave is distinct from the QRS complex and does not represent initial ventricular depolarization.
*Normal duration defined as less than 200 milliseconds*
- A duration of less than 200 milliseconds (0.20 seconds) typically refers to the normal duration of the **PR interval**, which represents atrial depolarization and conduction through the AV node.
- The **QRS complex** (initial ventricular depolarization) has a shorter normal duration, typically less than 120 milliseconds.
ACS US Medical PG Question 5: A 72-year-old man comes to the physician because of a 2-month history of intermittent retrosternal chest pain and tightness on exertion. He has type 2 diabetes mellitus, osteoarthritis of the right hip, and hypertension. Current medications include insulin, ibuprofen, enalapril, and hydrochlorothiazide. Vital signs are within normal limits. His troponin level is within the reference range. An ECG at rest shows a right bundle branch block and infrequent premature ventricular contractions. The patient's symptoms are reproduced during adenosine stress testing. Repeat ECG during stress testing shows new ST depression of > 1 mm in leads V2, V3, and V4. Which of the following is the most important underlying mechanism of this patient's ECG changes?
- A. Diversion of blood flow from stenotic coronary arteries (Correct Answer)
- B. Transient atrioventricular nodal blockade
- C. Reduced left ventricular preload
- D. Ruptured cholesterol plaque within a coronary vessel
- E. Increased myocardial oxygen demand
ACS Explanation: ***Diversion of blood flow from stenotic coronary arteries***
- The **adenosine stress test** induces **submaximal coronary vasodilation** in healthy vessels, diverting blood flow away from stenosed areas that are already maximally dilated, a phenomenon known as **coronary steal**.
- This **relative hypoperfusion** in areas supplied by stenotic arteries leads to myocardial ischemia, manifested as **new ST depression** on the ECG due to **subendocardial oxygen supply-demand mismatch**.
*Transient atrioventricular nodal blockade*
- While adenosine can cause transient AV nodal blockade, leading to AV blocks, this would manifest as specific changes in **PR interval** or **QRS drop-out**, not ST segment depression indicative of ischemia.
- The patient's symptoms and ECG changes point towards myocardial ischemia, not an AV conduction disturbance.
*Reduced left ventricular preload*
- Reduced preload can occur in certain cardiac conditions but is not the primary mechanism behind ST depression during an adenosine stress test.
- ECG changes due to reduced preload are usually nonspecific, such as **sinus tachycardia** or **low voltage**, and do not typically cause new ST depression in specific leads.
*Ruptured cholesterol plaque within a coronary vessel*
- A ruptured plaque with subsequent **thrombus formation** would lead to **acute coronary syndrome (ACS)**, characterized by persistent chest pain, **elevated troponins**, and potentially **ST elevation** or new **pathologic Q waves** if complete occlusion occurs.
- The patient's troponin level is normal, and his symptoms are intermittent and reproducible on stress testing, which is more consistent with **stable angina**.
*Increased myocardial oxygen demand*
- While increased myocardial oxygen demand is a component of angina pectoris, adenosine primarily causes **coronary vasodilation**, which can worsen ischemia in stenotic areas by diverting blood flow, rather than directly increasing myocardial oxygen demand itself.
- **Dobutamine stress testing** would be the test that primarily increases myocardial oxygen demand.
More ACS US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.