Thorax/Abdomen US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Thorax/Abdomen. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
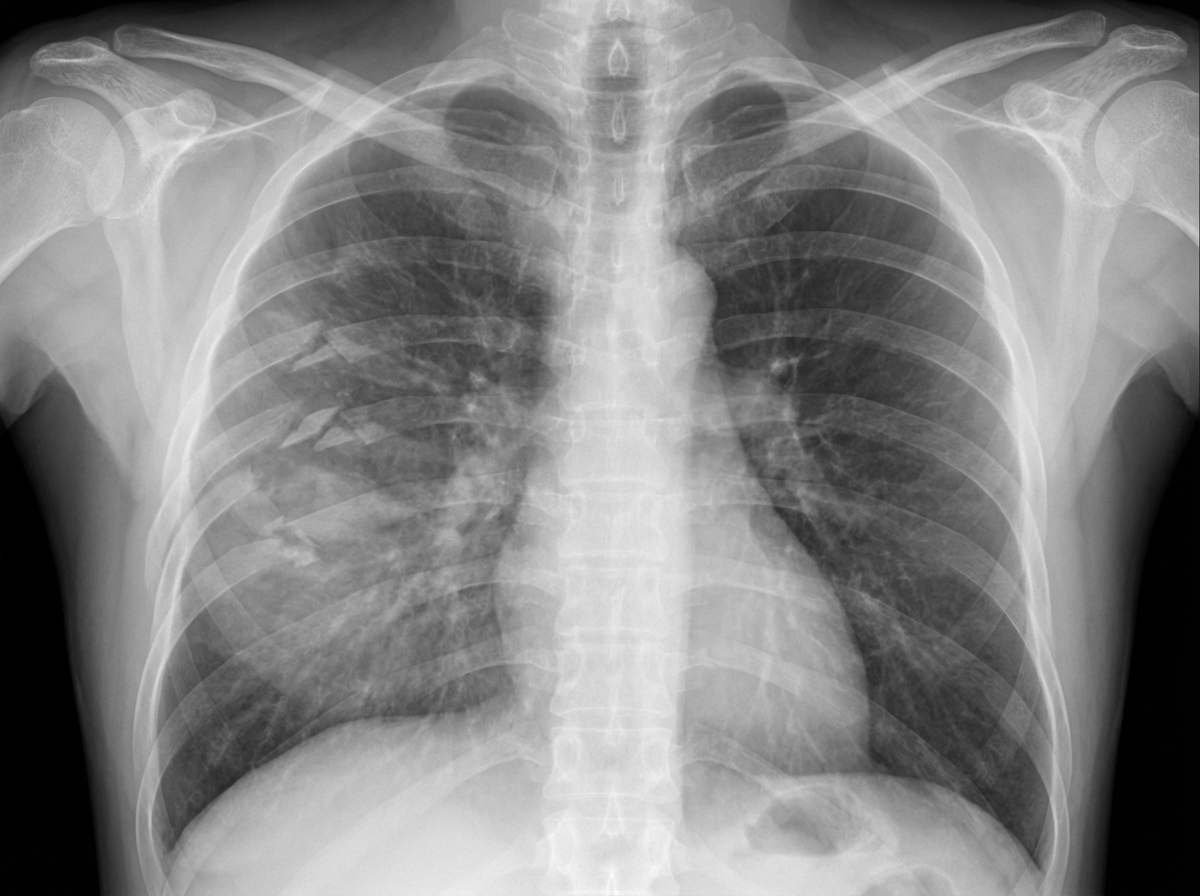
Thorax/Abdomen US Medical PG Question 1: A 27-year-old man is brought to the emergency department 45 minutes after being involved in a motor vehicle collision. He is agitated. He has pain in his upper right arm, which he is cradling in his left arm. His temperature is 36.7°C (98°F), pulse is 135/min, respirations are 25/min, and blood pressure is 145/90 mm Hg. His breathing is shallow. Pulse oximetry on 100% oxygen via a non-rebreather face mask shows an oxygen saturation of 83%. He is confused and oriented only to person. Examination shows multiple bruises on the right anterior thoracic wall. The pupils are equal and reactive to light. On inspiration, his right chest wall demonstrates paradoxical inward movement while his left chest wall is expanding. There is pain to palpation and crepitus over his right anterior ribs. The remainder of the examination shows no abnormalities. An x-ray of the chest is shown. Two large-bore IVs are placed. After fluid resuscitation and analgesia, which of the following is the most appropriate next step in management?
- A. Bedside thoracotomy
- B. Surgical fixation of right third to sixth ribs
- C. Intubation with positive pressure ventilation (Correct Answer)
- D. Placement of a chest tube
- E. CT scan of the chest
Thorax/Abdomen Explanation: ***Intubation with positive pressure ventilation***
- The patient presents with **flail chest** (paradoxical chest wall movement with pain and crepitus), respiratory distress (tachypnea, shallow breathing), and **hypoxemia** (SpO2 83% on 100% oxygen) despite initial fluid resuscitation and analgesia. These are clear indications for **endotracheal intubation** and mechanical ventilation to stabilize the chest wall, improve oxygenation, and reduce the work of breathing.
- **Positive pressure ventilation** helps to internally splint the flail segment, enabling more effective gas exchange and preventing further atelectasis.
*Bedside thoracotomy*
- **Bedside thoracotomy** is typically reserved for patients in traumatic cardiac arrest who have witnessed signs of life on arrival or are in profound shock unresponsive to other resuscitative measures, making it inappropriate here.
- This patient is **hemodynamically stable** (BP 145/90 mmHg) and does not show signs of massive hemorrhage or cardiac tamponade requiring immediate thoracotomy.
*Surgical fixation of right third to sixth ribs*
- **Surgical fixation of rib fractures** is a more definitive treatment for flail chest but is not an immediate life-saving intervention in the setting of acute respiratory failure and hypoxemia.
- While it can be considered later to reduce pain and improve pulmonary mechanics, the priority is to stabilize the patient's respiratory status through **ventilation**.
*Placement of a chest tube*
- **Placement of a chest tube** is indicated for pneumothorax, hemothorax, or empyema. While a pneumothorax or hemothorax could be present given the trauma and rib fractures, the primary issue driving this patient's acute respiratory failure is the **flail chest leading to inadequate ventilation and oxygenation**.
- There is no mention of diminished breath sounds or hyperresonance/dullness to percussion, which would suggest pneumothorax or hemothorax as the primary and immediate problem after initial resuscitation.
*CT scan of the chest*
- A **CT scan of the chest** is an important diagnostic tool to assess the extent of injuries, but it is not an immediate therapeutic intervention for a patient in acute respiratory failure and severe hypoxemia.
- Delaying definitive airway management for a diagnostic test in an unstable patient is **inappropriate** and could worsen the patient's condition.
Thorax/Abdomen US Medical PG Question 2: A 17-year-old boy presents to the emergency department for the evaluation of severe chest pain that started one hour ago. The pain suddenly began after he lifted a heavy object and the pain is constant. He has no history of a serious illness and takes no medications. His blood pressure is 125/85 mm Hg, the pulse is 89/min, the respiratory rate is 15/min, and the temperature is 36.7°C (98.1°F). Examination of the supraclavicular notch shows mild swelling of the skin with crepitation on palpation. Auscultation of the precordium in the left lateral decubitus position reveals a clicking sound with every heartbeat. The remainder of the physical examination shows no abnormalities. A chest X-ray is shown. Which of the following is the most appropriate next step in management?
- A. Needle aspiration
- B. Surgical exploration
- C. Supplemental oxygen (Correct Answer)
- D. Chest tube
- E. Video-assisted thoracoscopic surgery
Thorax/Abdomen Explanation: ***Supplemental oxygen***
- The patient's presentation with **sudden chest pain** after lifting a heavy object, **subcutaneous emphysema** (crepitation), and a pericardial **clicking sound (Hamman's sign)** suggests spontaneous pneumomediastinum.
- Though often benign and self-limiting, the initial management involves supportive care like **supplemental oxygen** for pain and improved oxygenation.
*Needle aspiration*
- This procedure is indicated for **tension pneumothorax**, which presents with respiratory distress, tracheal deviation, and hemodynamic instability, none of which are present here.
- Pneumomediastinum involves air in the mediastinum, not the pleural space, so needle aspiration of the pleural space would be ineffective and potentially harmful.
*Surgical exploration*
- Surgical exploration is rarely needed in spontaneous pneumomediastinum unless there is evidence of an **esophageal rupture** or another critical injury, or if conservative management fails.
- The patient's stable vital signs and lack of signs of septic shock or uncontrolled bleeding make immediate surgery unnecessary.
*Chest tube*
- A **chest tube** is used to drain air or fluid from the pleural space, typically for pneumothorax or pleural effusion.
- It is not indicated for isolated pneumomediastinum, as the air is in the mediastinum and not causing lung collapse.
*Video-assisted thoracoscopic surgery*
- **VATS** is a minimally invasive surgical procedure that might be used for persistent air leaks, recurrent pneumothorax, or for diagnosis and treatment of conditions like esophageal rupture, which are not suggested by this patient's presentation.
- Given the isolated pneumomediastinum, conservative management is the first-line treatment.
Thorax/Abdomen US Medical PG Question 3: A 72-year-old man presents to the emergency department after a fall. The patient was found lying down on the floor in his room in his retirement community. The patient has a past medical history of Alzheimer dementia and a prosthetic valve. His current medications include donepezil and warfarin. His temperature is 97.7°F (36.5°C), blood pressure is 85/50 mmHg, pulse is 160/min, respirations are 13/min, and oxygen saturation is 97% on room air. The patient is started on IV fluids and a type and screen is performed. Laboratory values are ordered as seen below.
Hemoglobin: 13 g/dL
Hematocrit: 39%
Leukocyte count: 5,500 cells/mm^3 with normal differential
Platelet count: 225,000/mm^3
INR: 2.5
AST: 10 U/L
ALT: 12 U/L
A chest radiograph and EKG are performed and are within normal limits. A full physical exam is within normal limits. The patient's vitals are repeated. His temperature is 99.5°F (37.5°C), blood pressure is 110/70 mmHg, pulse is 90/min, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
- A. CT scan (Correct Answer)
- B. Urgent blood transfusion
- C. Fresh frozen plasma
- D. Exploratory laparoscopy
- E. Exploratory laparotomy
Thorax/Abdomen Explanation: ***CT scan***
- A patient with a **prosthetic valve** on **warfarin** and a fall is at high risk for **intracranial hemorrhage**, even without focal neurological deficits.
- While initial vitals improved after IV fluids, the mechanism of injury (fall) and medication profile warrant a **CT scan** of the head to rule out serious internal injury, especially given the history of dementia which might mask symptoms.
*Urgent blood transfusion*
- The patient's **hemoglobin (13 g/dL)** and **hematocrit (39%)** are within normal limits, indicating no acute need for blood transfusion due to hemorrhage.
- Transfusions are typically reserved for patients with significant blood loss or severe symptomatic anemia.
*Fresh frozen plasma*
- The patient's **INR of 2.5** is within the therapeutic range for a patient with a prosthetic valve on warfarin.
- There is no evidence of active bleeding or supratherapeutic anticoagulation that would necessitate the administration of **fresh frozen plasma (FFP)** to reverse anticoagulation.
*Exploratory laparoscopy*
- There are no clinical signs or symptoms, such as abdominal pain, distension, or evidence of intra-abdominal bleeding (e.g., declining hemoglobin, peritoneal signs), to suggest an indication for an **exploratory laparoscopy**.
- The patient's physical exam was described as normal.
*Exploratory laparotomy*
- Similar to laparoscopy, there is no clinical evidence of acute abdominal injury or hemorrhage, which would necessitate an **exploratory laparotomy**.
- This invasive procedure is reserved for cases with strong suspicion of significant intra-abdominal pathology or trauma.
Thorax/Abdomen US Medical PG Question 4: A 71-year-old man is admitted to the hospital one hour after he was found unconscious. His pulse is 80/min and systolic blood pressure is 98 mm Hg; diastolic blood pressure cannot be measured. He is intubated and mechanically ventilated with supplemental oxygen at a tidal volume of 450 mL and a respiratory rate of 10/min. Arterial blood gas analysis shows:
PCO2 43 mm Hg
O2 saturation 94%
O2 content 169 mL/L
Pulmonary artery catheterization shows a pulmonary artery pressure of 15 mm Hg and a pulmonary capillary wedge pressure of 7 mm Hg. Bedside indirect calorimetry shows a rate of O2 tissue consumption of 325 mL/min. Given this information, which of the following additional values is sufficient to calculate the cardiac output in this patient?
- A. Left ventricular end-diastolic volume
- B. Partial pressure of inspired oxygen
- C. End-tidal carbon dioxide pressure
- D. Pulmonary artery oxygen content (Correct Answer)
- E. Total peripheral resistance
Thorax/Abdomen Explanation: ***Pulmonary artery oxygen content***
- Cardiac output can be calculated using the **Fick principle**, which states that **Cardiac Output = (Oxygen Consumption) / (Arteriovenous Oxygen Difference)**.
- We are provided with **O2 tissue consumption (325 mL/min)** and **arterial O2 content (169 mL/L)**. To complete the Fick equation, we need the **mixed venous oxygen content**, which is represented by the **pulmonary artery oxygen content**.
*Left ventricular end-diastolic volume*
- While **left ventricular end-diastolic volume** is a determinant of stroke volume (and thus cardiac output), it alone is not sufficient to calculate cardiac output without knowing heart rate and ejection fraction.
- This value is more relevant for assessing **preload** and ventricular function.
*Partial pressure of inspired oxygen*
- The **partial pressure of inspired oxygen** is used to calculate the **alveolar oxygen partial pressure** and is important for assessing oxygenation and respiratory function.
- It is not directly used in the Fick principle for calculating cardiac output.
*End-tidal carbon dioxide pressure*
- **End-tidal carbon dioxide (ETCO2)** is a measure of the partial pressure of CO2 at the end of exhalation and reflects ventilation and pulmonary perfusion.
- While it can be correlated with cardiac output in certain clinical contexts, it is not a direct input for the **Fick principle** calculation of cardiac output.
*Total peripheral resistance*
- **Total peripheral resistance (TPR)** can be calculated from cardiac output and mean arterial pressure using the formula: **(MAP - CVP) / CO**, but it cannot be used to calculate cardiac output directly without knowing the other variables.
- TPR is a measure of the **resistance to blood flow** in the systemic circulation.
Thorax/Abdomen US Medical PG Question 5: A 32-year-old woman comes to the physician for a screening health examination that is required for scuba diving certification. The physician asks her to perform a breathing technique: following deep inspiration, she is instructed to forcefully exhale against a closed airway and contract her abdominal muscles while different cardiovascular parameters are evaluated. Which of the following effects is most likely after 10 seconds in this position?
- A. Decreased intra-abdominal pressure
- B. Decreased left ventricular stroke volume (Correct Answer)
- C. Decreased pulse rate
- D. Decreased systemic vascular resistance
- E. Increased venous return to left atrium
Thorax/Abdomen Explanation: ***Decreased left ventricular stroke volume***
- After 10 seconds of performing the **Valsalva maneuver**, the increased intrathoracic pressure significantly reduces **venous return** to the heart.
- Reduced venous return leads to decreased **ventricular filling** (preload), which in turn diminishes **left ventricular stroke volume** and cardiac output.
*Decreased intra-abdominal pressure*
- The instruction to "contract her abdominal muscles" during forceful exhalation against a closed airway (Valsalva maneuver) directly leads to an **increase** in **intra-abdominal pressure**, not a decrease.
- This increase in intra-abdominal pressure further impedes venous return from the lower extremities to the heart.
*Decreased pulse rate*
- In the initial phase of the Valsalva maneuver (first 5-10 seconds), the decrease in cardiac output triggers a **reflex tachycardia** to maintain blood pressure, leading to an **increased pulse rate**.
- A decrease in pulse rate (bradycardia) is more characteristic of the release phase, not during the sustained strain.
*Decreased systemic vascular resistance*
- During the Valsalva maneuver, the body attempts to compensate for the drop in cardiac output and blood pressure by increasing **sympathetic tone**, which causes **vasoconstriction** and thus **increases systemic vascular resistance**.
- A decrease in systemic vascular resistance would further drop blood pressure and is not the physiological response during this phase.
*Increased venous return to left atrium*
- The Valsalva maneuver dramatically **reduces venous return** to both the right and left atria due to the high intrathoracic pressure compressing the great veins.
- This decreased venous return is the primary mechanism leading to the subsequent fall in cardiac output during the maneuver.
More Thorax/Abdomen US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.