
Respiratory System
Complete Respiratory System study resources for NEET-PG. Part of Physiology.
Study Resources
Choose how you want to study Respiratory System
Lessons
10 lessons in Respiratory System

Mechanics of Breathing

Pulmonary Ventilation

Pulmonary Circulation
Master Pulmonary Circulation for NEET-PG & INI-CET. Free high-yield physiology notes on low pressure dynamics, HPV, and V/Q matching. Ace your exams!

Gas Exchange in the Lungs

Oxygen and Carbon Dioxide Transport

Control of Breathing

Respiratory Adjustments in Health and Disease

High Altitude Physiology

Diving Physiology

Respiratory Function Tests
Practice Questions
10 MCQs for Respiratory System
Sample Questions: Respiratory System
Test your understanding with these related questions
A 68-year-old man with both severe COPD (emphysema) and newly diagnosed idiopathic pulmonary fibrosis presents with worsening dyspnea. His pressure-volume curve shows a complex pattern with features of both diseases. Static compliance measured at mid-lung volumes is 120 mL/cm H2O. His pulmonologist must decide on optimal management. Synthesizing the pathophysiology of both conditions, what represents the most significant clinical challenge in managing his combined disease?
Respiratory System Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Respiratory System. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Respiratory System Indian Medical PG Question 1: A 68-year-old man with both severe COPD (emphysema) and newly diagnosed idiopathic pulmonary fibrosis presents with worsening dyspnea. His pressure-volume curve shows a complex pattern with features of both diseases. Static compliance measured at mid-lung volumes is 120 mL/cm H2O. His pulmonologist must decide on optimal management. Synthesizing the pathophysiology of both conditions, what represents the most significant clinical challenge in managing his combined disease?
- A. The opposing effects on compliance create a pseudonormal total respiratory compliance masking disease severity (Correct Answer)
- B. Emphysema treatment with bronchodilators will worsen fibrosis progression
- C. Pulmonary rehabilitation cannot address the opposing mechanical derangements
- D. The increased compliance from emphysema completely negates decreased compliance from fibrosis
- E. Oxygen therapy beneficial for COPD will accelerate fibrotic changes
Respiratory System Explanation: ***The opposing effects on compliance create a pseudonormal total respiratory compliance masking disease severity*** - In **Combined Pulmonary Fibrosis and Emphysema (CPFE)**, the high compliance of **emphysema** (loss of elastic recoil) and low compliance of **fibrosis** (increased stiffness) mathematically offset each other. - This leads to **pseudonormalization** of lung volumes (like FVC or TLC) and static compliance, which can dangerously mask the physiologic severity and lead to delayed clinical intervention. *Emphysema treatment with bronchodilators will worsen fibrosis progression* - **Bronchodilators** target airway smooth muscle tone and do not have a known mechanistic pathway to accelerate **collagen deposition** or fibroblast activation in the interstitium. - Standard therapy for the **obstructive component** of COPD is generally safe to use in patients who also have concurrent interstitial lung disease. *Pulmonary rehabilitation cannot address the opposing mechanical derangements* - While **pulmonary rehabilitation** cannot physically reverse the mechanical changes in the lung tissue, it is highly effective at improving **skeletal muscle efficiency** and dyspnea perception. - It remains a cornerstone of management for both **restrictive and obstructive** diseases by optimizing the patient's functional capacity despite lung damage. *The increased compliance from emphysema completely negates decreased compliance from fibrosis* - While the mechanics are opposing, they rarely "completely negate" one another; rather, they result in severe **gas exchange impairment** (profoundly low DLCO) out of proportion to the spirometry. - High-resolution CT usually shows distinct regional differences, typically **upper-lobe emphysema** and **lower-lobe fibrosis**, rather than a uniform mechanical cancellation. *Oxygen therapy beneficial for COPD will accelerate fibrotic changes* - Standard **supplemental oxygen** used to maintain target saturations does not trigger or accelerate the **pathogenesis of idiopathic pulmonary fibrosis**. - Oxygen is essential for managing **pulmonary hypertension**, which is a frequent and severe complication in patients with the combined CPFE phenotype.
Respiratory System Indian Medical PG Question 2: A 42-year-old woman with systemic sclerosis develops both pulmonary fibrosis and chest wall restriction from skin thickening. Her measured total respiratory system compliance is 30 mL/cm H2O. Testing with complete paralysis and positive pressure ventilation shows isolated lung compliance of 50 mL/cm H2O. She is being considered for immunosuppressive therapy versus supportive care. Evaluate which intervention would provide the greatest improvement in her respiratory mechanics.
- A. Aggressive immunosuppression targeting both lung and skin disease
- B. Lung-directed therapy only, as it contributes more to total compliance reduction
- C. Supportive care only, as both components contribute equally and irreversibly
- D. Combined therapy targeting lung disease with chest wall mobilization (Correct Answer)
- E. Chest wall-directed physical therapy, as it is the primary limiting factor
Respiratory System Explanation: ***Combined therapy targeting lung disease with chest wall mobilization*** - Total respiratory compliance (30 mL/cm H₂O) is determined by the formula **1/C_total = 1/C_lung + 1/C_chest wall**; calculating this yields a **chest wall compliance (C_cw)** of 75 mL/cm H₂O. - Since both **C_lung (50 mL/cm H₂O)** and **C_cw (75 mL/cm H₂O)** are significantly lower than the normal value of ~200 mL/cm H₂O, addressing both the **interstitial lung disease** and the **extrapulmonary restriction** is necessary. *Aggressive immunosuppression targeting both lung and skin disease* - While immunosuppression may slow **fibrotic progression**, it often fails to immediately or significantly reverse the **mechanical restriction** caused by established chest wall skin thickening. - This approach neglects the physical aspect of **chest wall mobilization** required to improve the compliance of the thoracic cage. *Lung-directed therapy only, as it contributes more to total compliance reduction* - Measured **C_lung (50)** is indeed lower than **C_cw (75)**, but the total work of breathing is significantly impacted by the sum of these **resistances**. - Ignoring the **chest wall component** limits the potential improvement in **vital capacity** and respiratory efficiency. *Supportive care only, as both components contribute equally and irreversibly* - Systemic sclerosis-related **pulmonary fibrosis** and **skin tightening** are not necessarily irreversible; early intervention can stabilize or improve lung function. - This pessimistic view ignores that **C_cw** can be improved through **rehabilitation** and that **C_lung** can be managed with modern **immunosuppressive protocols**. *Chest wall-directed physical therapy, as it is the primary limiting factor* - This is incorrect as the **C_lung (50 mL/cm H₂O)** is actually more impaired than the **C_cw (75 mL/cm H₂O)**. - Focusing solely on the chest wall ignores the **significant parenchymal disease** which is the more dominant factor in this patient's **restrictive physiology**.
Respiratory System Indian Medical PG Question 3: A 58-year-old man with end-stage pulmonary fibrosis is being evaluated for lung transplantation. His current static compliance is 25 mL/cm H2O (normal: 200 mL/cm H2O). He also has mild obesity (BMI 32) and ankylosing spondylitis affecting chest wall mobility. Post-transplant, assuming successful bilateral lung transplant with normal donor lungs, what would be the expected change in his total respiratory system compliance?
- A. Return to completely normal respiratory compliance matching healthy individuals
- B. Improved but still reduced compliance due to persistent chest wall restriction (Correct Answer)
- C. Improved lung compliance but worsened chest wall compliance from surgery
- D. Worse compliance initially due to transplant rejection and denervation
- E. No significant change because the primary problem is muscular weakness
Respiratory System Explanation: ***Improved but still reduced compliance due to persistent chest wall restriction*** - Total respiratory system compliance is determined by the **inverse sum of lung and chest wall compliance** (1/Ct = 1/Cl + 1/Ccw). - While the transplant provides **normal lung compliance**, the patient has extrinsic restrictions from **obesity** and **ankylosing spondylitis** that keep the chest wall compliance low. *Return to completely normal respiratory compliance matching healthy individuals* - Total compliance cannot return to normal because the **extrapulmonary constraints** (stiff chest wall and adipose tissue) are not altered by the surgery. - The **ankylosing spondylitis** specifically limits the expansion of the thoracic cage, regardless of how healthy the new lungs are. *Improved lung compliance but worsened chest wall compliance from surgery* - While surgical trauma can cause temporary pain, a successful transplant doesn't inherently **permanently worsen** pre-existing chest wall stiffness. - The primary physiological takeaway is the **net improvement** in one component (lungs) while the other remains a fixed restrictive limiting factor. *Worse compliance initially due to transplant rejection and denervation* - **Denervation** of the lung does not significantly decrease its static compliance; its elasticity is primarily due to its **structural parenchyma**. - While **rejection** could decrease compliance, the question asks for the expected change assuming a **successful transplant** with normal donor tissue. *No significant change because the primary problem is muscular weakness* - The primary problem in this case is **structural restriction** (fibrosis and chest wall stiffening) rather than neuromuscular transmission or muscular weakness. - Correcting end-stage **pulmonary fibrosis** will always provide a significant increase in total compliance, even if the result remains below the physiological norm.
Respiratory System Indian Medical PG Question 4: A research study compares two patients with different lung pathologies but identical functional residual capacity (FRC) of 3.0 L. Patient A has pulmonary fibrosis with FRC above the steep portion of the compliance curve. Patient B has emphysema with FRC on the flat upper portion of the curve. Both attempt to inhale the same tidal volume. Analyzing their work of breathing, which statement best characterizes the difference?
- A. Patient A does more elastic work; Patient B does more resistive work
- B. Patient B does more elastic work due to hyperinflation beyond optimal compliance (Correct Answer)
- C. Patient B does less work because emphysematous lungs are more compliant
- D. Patient A does less work because fibrotic lungs have increased elastic recoil assisting inspiration
- E. Both do equal work because FRC and tidal volumes are identical
Respiratory System Explanation: ***Patient B does more elastic work due to hyperinflation beyond optimal compliance*** - Although **emphysema** creates high compliance at low volumes, the patient in this scenario is at a high **FRC** on the **flat upper portion** of the compliance curve where the lung is already overstretched. - At this point, additional expansion requires significantly higher pressure changes for the same volume, drastically increasing the **elastic work of breathing** due to **hyperinflation** and loss of mechanical advantage. *Patient A does more elastic work; Patient B does more resistive work* - **Patient A** (fibrosis) does have high elastic work due to stiff lungs, but the question specifies **Patient B** is on the flat, non-compliant portion of the curve where elastic work becomes excessive. - **Resistive work** is primarily associated with **airway obstruction** during expiration, while this specific comparison focuses on the **pressure-volume** (elastic) dynamics of inspiration. *Patient B does less work because emphysematous lungs are more compliant* - While **emphysematous lungs** have increased static compliance, they become functionally **non-compliant** at high lung volumes near total lung capacity (**TLC**). - Operating on the **flat upper portion** of the curve means the lungs are near their limit of distensibility, requiring more effort, not less, to achieve a **tidal volume**. *Patient A does less work because fibrotic lungs have increased elastic recoil assisting inspiration* - In **pulmonary fibrosis**, increased **elastic recoil** actually opposes inspiration, making the lungs stiffer and requiring more work to expand. - **Elastic recoil** assists expiration, not inspiration; therefore, **fibrotic lungs** always require significantly more work to inflate compared to healthy lungs. *Both do equal work because FRC and tidal volumes are identical* - Identical **FRC** and **tidal volumes** do not imply equal work if the patients are operating on different phases of the **pressure-volume curve**. - The **work of breathing** is determined by the area under the pressure-volume loop, which is dictated by the **lung compliance** at that specific starting volume.
Respiratory System Indian Medical PG Question 5: A 32-year-old woman develops acute respiratory distress syndrome (ARDS) following sepsis. She is mechanically ventilated with tidal volume 450 mL and plateau pressure 35 cm H2O (PEEP 10 cm H2O). Her static compliance is calculated as 18 mL/cm H2O. The team considers changing ventilator settings. Analyzing her respiratory mechanics, what change would most effectively improve compliance while minimizing ventilator-induced lung injury?
- A. Increase tidal volume to 600 mL to recruit more alveoli
- B. Decrease PEEP to 5 cm H2O to reduce plateau pressure
- C. Switch to pressure-control mode with same plateau pressure
- D. Increase respiratory rate while maintaining current tidal volume
- E. Increase PEEP to 15 cm H2O to prevent alveolar collapse (Correct Answer)
Respiratory System Explanation: ***Increase PEEP to 15 cm H2O to prevent alveolar collapse*** - In **ARDS**, static compliance is low due to widespread **alveolar collapse**; increasing **PEEP** (Positive End-Expiratory Pressure) recruits collapsed alveoli and shifts the lung to a more compliant part of the **pressure-volume curve**. - Preventing cyclic collapse (atelectrauma) through adequate PEEP minimizes **Ventilator-Induced Lung Injury (VILI)** while effectively improving gas exchange area and lung mechanics. *Increase tidal volume to 600 mL to recruit more alveoli* - High tidal volumes increase the risk of **volutrauma** and **overdistension** of relatively healthy alveoli (the "baby lung" concept in ARDS). - This action would likely increase the **plateau pressure** further above the 30 cm H2O safety threshold, worsening lung injury. *Decrease PEEP to 5 cm H2O to reduce plateau pressure* - Reducing PEEP below the **lower inflection point** leads to **atelectrauma** via the repeated opening and closing of unstable alveoli. - While it might lower peak pressures, it would cause a drop in functional residual capacity and a significant decrease in **static compliance**. *Switch to pressure-control mode with same plateau pressure* - Simply switching to **pressure-control ventilation** does not inherently change the underlying **respiratory mechanics** or lung compliance if the plateau pressure remains constant. - Without addressing alveolar recruitment through PEEP, the **compliance** remains compromised by the disease process itself. *Increase respiratory rate while maintaining current tidal volume* - Increasing the **respiratory rate** may help manage hypercapnia but does not directly improve the **static compliance** of the lung tissue. - High rates can lead to **auto-PEEP** or intrinsic PEEP, which can complicate the assessment of plateau pressures and hemodynamics.
More Respiratory System Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.
Flashcards
10 cards for Respiratory System
Sample Flashcards: Respiratory System
The graph given below shows _____ _____thoracic obstruction
Hint: variable/fixed
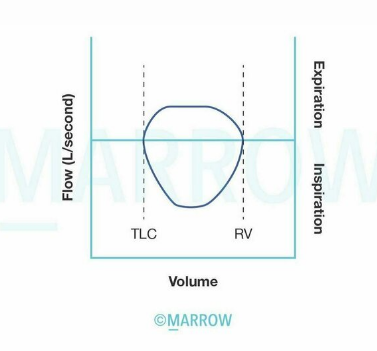
The graph given below shows _____ _____thoracic obstruction
variable
Respiratory System Flashcards - Medical Study Cards by OnCourse
Master Respiratory System with OnCourse flashcards. These spaced repetition flashcards are designed for medical students preparing for NEET PG, USMLE Step 1, USMLE Step 2, MBBS exams, and other medical licensing examinations.
OnCourse flashcards use active recall and spaced repetition techniques similar to Anki to help you memorize and retain medical concepts effectively. Each card is crafted by medical experts to cover high-yield topics.
Why use OnCourse Flashcards for Respiratory System?
- Spaced repetition algorithm for optimal retention
- Anki-style cloze deletions for active recall
- Created by medical professionals and educators
- Covers NEET PG, USMLE, PLAB, and MBBS curricula
- Mobile app available for studying on the go
Respiratory System Flashcard Deck - 5 Cards
Respiratory System Flashcard 1 of 5
Question: The graph given below shows _____ _____thoracic obstruction
Answer: variable
Respiratory System Flashcard 2 of 5
Question: The graph given depicts the _____ effect
Answer: Haldane
Respiratory System Flashcard 3 of 5
Question: The alveolar gas equation states that the alveolar Po2 (PAo2) equals: _____
Answer:
Respiratory System Flashcard 4 of 5
Question: According to Fick's law, the rate of diffusion of a gas (Vgas) is equal to: _____
Answer:
Respiratory System Flashcard 5 of 5
Question: What equation may be used to determine the physiologic dead space (VD)? _____
Answer:
Download the OnCourse app to access all 5 flashcards for Respiratory System, plus thousands more covering Anatomy, Physiology, Pathology, Pharmacology, Microbiology, Biochemistry, and all medical subjects. Better than Anki for medical students!
Keywords: Respiratory System flashcards, medical flashcards, NEET PG preparation, USMLE Step 1 flashcards, Anki alternative, spaced repetition medical, OnCourse flashcards, medical exam preparation, MBBS study material, active recall medical education
Have doubts about this lesson?
Ask Rezzy, our AI tutor, to explain anything you didn't understand
About Respiratory System for NEET-PG
Respiratory System is a key topic within Physiology for NEET-PG preparation. OnCourse provides 10 comprehensive lessons, 10 practice MCQs, and 10 flashcards to help you master this topic.
Lessons in Respiratory System
- Mechanics of Breathing
- Pulmonary Ventilation
- Pulmonary Circulation
- Gas Exchange in the Lungs
- Oxygen and Carbon Dioxide Transport
- Control of Breathing
- Respiratory Adjustments in Health and Disease
- High Altitude Physiology
- Diving Physiology
- Respiratory Function Tests
Part of Physiology for NEET-PG preparation on OnCourse.
Master Respiratory System
Get full access to all 10 lessons, 10 questions, and AI-powered study tools.
Start For Free