Neoplasia Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Neoplasia. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Neoplasia Indian Medical PG Question 1: What is the most common carcinoma to develop after burns?
- A. Squamous cell carcinoma (Correct Answer)
- B. Adenocarcinoma
- C. Melanoma
- D. Mucoid carcinoma
Neoplasia Explanation: **Explanation:**
The correct answer is **Squamous Cell Carcinoma (SCC)**. This specific clinical scenario refers to a **Marjolin’s ulcer**, which is a malignancy arising in a chronic non-healing wound, scar tissue, or most classically, a **long-standing burn scar** [1].
**Why it is correct:**
Chronic irritation, persistent inflammation, and repeated trauma to a burn scar lead to constant cellular turnover. Over time, the damaged skin undergoes malignant transformation. In the skin, the predominant cell type is the keratinocyte; therefore, the resulting malignancy is almost always Squamous Cell Carcinoma [1]. Marjolin’s ulcers are typically more aggressive and have a higher rate of metastasis than SCC arising from sun-damaged skin.
**Why other options are incorrect:**
* **B. Adenocarcinoma:** This arises from glandular epithelium (e.g., GI tract, breast, lung). Skin lacks the primary glandular structures required for this to be a common post-burn complication.
* **C. Melanoma:** While melanoma arises from melanocytes in the skin, it is associated with UV radiation and genetic factors rather than chronic scarring or thermal injury.
* **D. Mucoid carcinoma:** This is a variant of adenocarcinoma (often seen in the breast or GI tract) characterized by abundant mucin production; it has no association with burn scars.
**High-Yield Pearls for NEET-PG:**
* **Marjolin’s Ulcer:** The classic triad is a chronic scar, a non-healing ulcer, and Squamous Cell Carcinoma [1].
* **Latent Period:** The average time from the initial burn to the development of SCC is often **20–30 years**.
* **Other associations:** Marjolin’s ulcers can also develop in chronic osteomyelitis sinuses and venous stasis ulcers [1].
* **Diagnosis:** Always perform a biopsy on any ulcerating lesion appearing in an old scar.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Disorders Involving Inflammatory And Haemopoietic Cells, pp. 644-645.
Neoplasia Indian Medical PG Question 2: A female patient presents with a 2 x 2 cm firm mass in the upper outer quadrant of the breast. She has a family history of ovarian carcinoma. Which investigation needs to be done to assess for a specific gene mutation?
- A. p53
- B. BRCA-2 (Correct Answer)
- C. Her 2/Neu gene
- D. C-myc gene
Neoplasia Explanation: ### Explanation
**Correct Option: B (BRCA-2)**
The clinical presentation of a breast mass in a patient with a strong family history of ovarian carcinoma strongly suggests **Hereditary Breast and Ovarian Cancer (HBOC) syndrome**. [1]
* **BRCA-1 and BRCA-2** are tumor suppressor genes involved in DNA repair (homologous recombination). [1]
* While both increase the risk of breast and ovarian cancer, **BRCA-2** is specifically associated with a higher risk of male breast cancer and is frequently tested when there is a strong clustering of these two specific malignancies in a family. In the context of this question, it is the most specific marker for the dual risk of breast and ovarian carcinoma.
**Why other options are incorrect:**
* **A. p53:** Mutations in p53 are associated with **Li-Fraumeni Syndrome**. While this increases breast cancer risk, it typically presents with a broader spectrum of tumors (Sarcomas, Brain tumors, Leukemia, and Adrenocortical carcinoma) rather than a specific breast-ovarian link. [2]
* **C. Her 2/Neu:** This is a proto-oncogene (ERBB2). Testing is done for **prognosis and treatment stratification** (Trastuzumab therapy) in confirmed cases, but it is a somatic mutation, not a germline mutation used to assess familial predisposition. [2]
* **D. C-myc:** This oncogene is primarily associated with **Burkitt Lymphoma** (t(8;14)). It does not have a primary diagnostic role in familial breast-ovarian cancer syndromes.
**High-Yield Clinical Pearls for NEET-PG:**
* **BRCA-1 Location:** Chromosome 17q21.
* **BRCA-2 Location:** Chromosome 13q12.3.
* **Most common breast cancer type in BRCA-1:** Triple Negative (Basal-like).
* **Most common breast cancer type in BRCA-2:** ER positive (Luminal). [2]
* **Other BRCA-2 associations:** Prostate, Pancreatic, and Gallbladder cancer. [1]
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Breast, pp. 1058-1059.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Breast, pp. 1059-1060.
Neoplasia Indian Medical PG Question 3: Which of the following conditions is not considered a premalignant condition?
- A. Erosive lichen planus
- B. Syphilitic glossitis
- C. Leukoedema (Correct Answer)
- D. Leukoplakia
Neoplasia Explanation: **Explanation:**
The core concept in this question is distinguishing between **potentially malignant disorders (PMDs)** and **normal anatomical variations** of the oral mucosa.
**Why Leukoedema is the correct answer:**
Leukoedema is a **benign, physiological variation** of the oral mucosa, not a premalignant condition. It is characterized by a diffuse, greyish-white, milky opalescence of the buccal mucosa that **disappears when the tissue is stretched** (a key diagnostic feature). Histologically, it shows intracellular edema of the spinous layer but lacks cellular atypia or dysplasia. It has no potential for malignant transformation.
**Analysis of Incorrect Options:**
* **Erosive Lichen Planus:** While the reticular form has a very low risk, the **erosive and atrophic forms** of Oral Lichen Planus are recognized as premalignant conditions with a transformation rate of approximately 1-2%.
* **Syphilitic Glossitis:** Chronic interstitial glossitis in tertiary syphilis is a classic premalignant condition. The associated atrophy and chronic inflammation of the tongue dorsum significantly increase the risk of squamous cell carcinoma.
* **Leukoplakia:** This is the **most common** premalignant lesion of the oral cavity [1]. It is a clinical term for a white patch that cannot be rubbed off or characterized as any other disease [1]. The risk of malignancy depends on the degree of dysplasia.
**High-Yield Clinical Pearls for NEET-PG:**
* **Leukoedema:** Most common in African Americans and smokers; "disappears on stretching" is the pathognomonic clinical sign.
* **Highest Malignant Potential:** Among oral lesions, **Erythroplakia** (red patch) has a much higher risk of malignancy (up to 90% show dysplasia/carcinoma) compared to Leukoplakia.
* **Speckled Leukoplakia:** Also known as Erythroleukoplakia, it carries a higher risk than homogenous leukoplakia.
* **Other PMDs:** Oral Submucous Fibrosis (OSMF) and Sideropenic Dysphagia (Plummer-Vinson Syndrome) are other high-yield premalignant conditions.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 344-345.
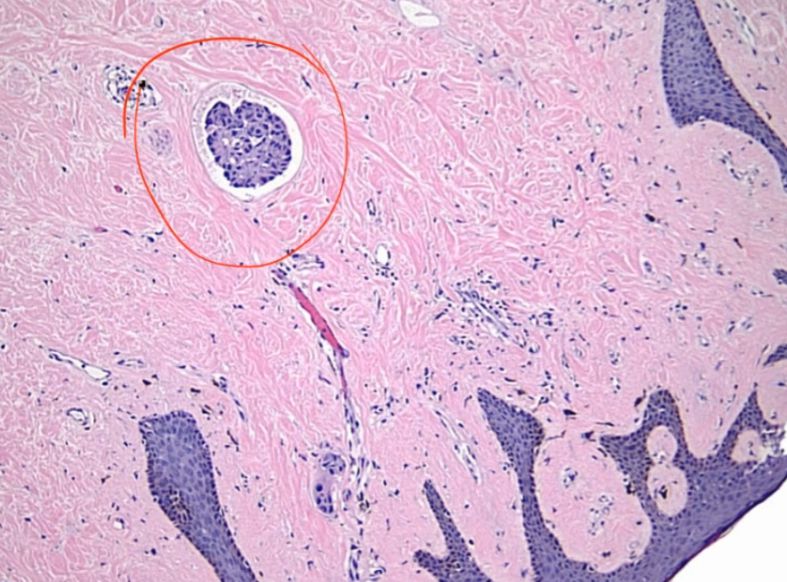
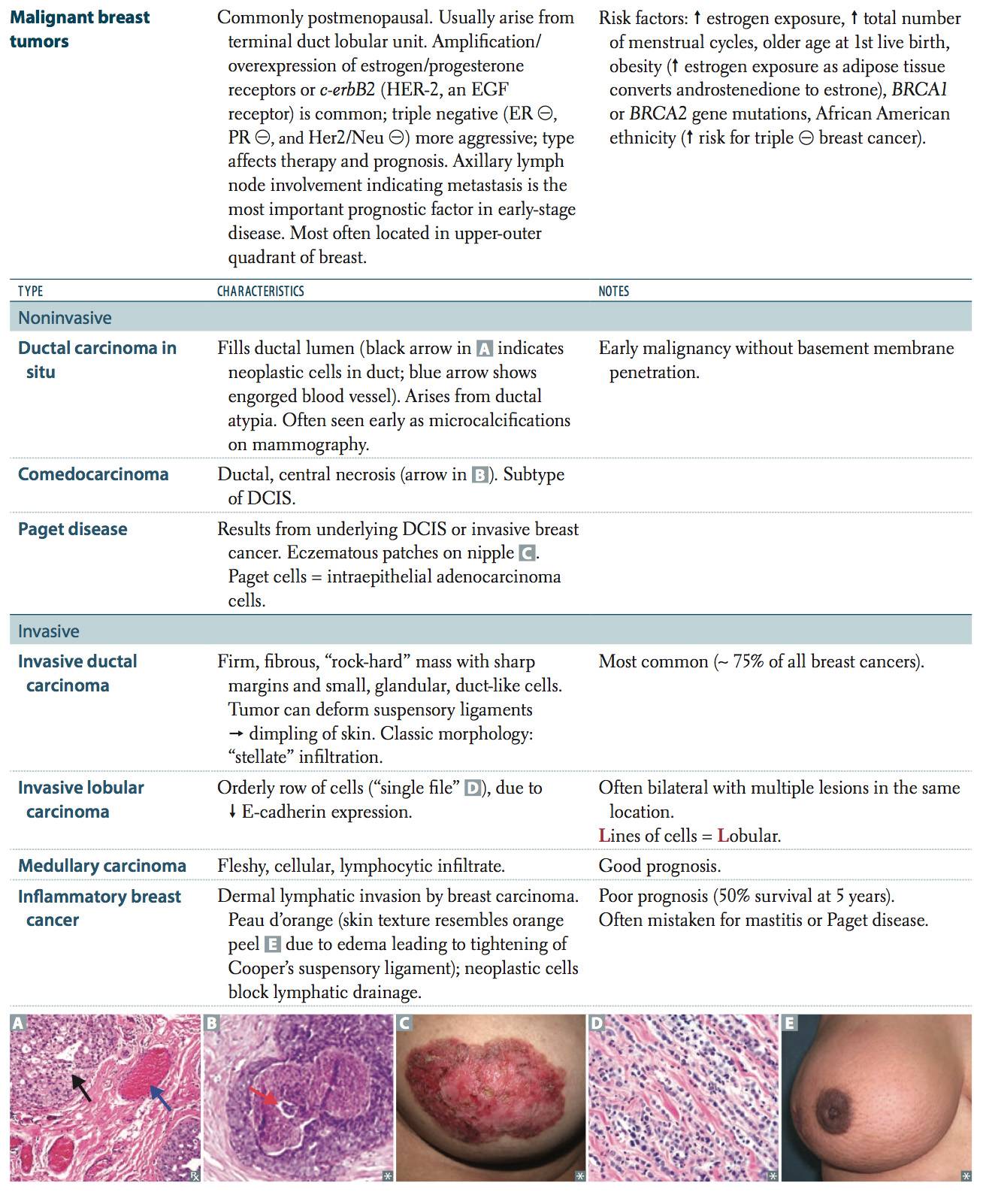
Neoplasia Indian Medical PG Question 4: A 55-year-old female presents with swollen, red, and tender right breast. The physician palpates a firm area and suspects inflammatory breast cancer. Which of the following best describes the histological changes observed in this disorder?
- A. Acute inflammation in breast carcinoma
- B. Chronic inflammation in breast carcinoma
- C. Dermal lymphatic invasion by cancer cells (Correct Answer)
- D. Epidermal invasion by cancer cells
Neoplasia Explanation: ### Explanation
**1. Why the Correct Answer is Right:**
The clinical presentation of a swollen, red, and tender breast (mimicking mastitis) in an older female is a classic description of **Inflammatory Breast Cancer (IBC)**. Despite the name, the "inflammatory" appearance is not due to an underlying infection or leukocyte infiltration. Instead, it is caused by **tumor emboli obstructing the dermal lymphatic channels**. This obstruction leads to lymphatic congestion and lymphedema, which manifests clinically as the characteristic **"Peau d'orange"** (orange peel) appearance of the skin [1].
**2. Why the Incorrect Options are Wrong:**
* **Options A & B:** While the breast appears clinically inflamed (rubor, tumor, calor), the underlying pathology is **not** an infiltration of acute (neutrophils) or chronic (lymphocytes/plasma cells) inflammatory cells. It is a mechanical blockage of lymphatics by malignant cells.
* **Option D:** Epidermal invasion by cancer cells is characteristic of **Paget’s Disease of the Breast**, where malignant cells (Paget cells) migrate from an underlying ductal carcinoma in situ (DCIS) into the nipple epidermis, causing an eczematous, crusting lesion.
**3. High-Yield Clinical Pearls for NEET-PG:**
* **Clinical Diagnosis:** IBC is a clinical-pathologic diagnosis. If a patient suspected of having mastitis does not respond to a course of antibiotics, a biopsy is mandatory to rule out IBC.
* **Prognosis:** IBC is highly aggressive (T4d in TNM staging) and is considered Stage IIIB or IV at the time of diagnosis.
* **Peau d'orange:** This occurs because the skin is tethered by the suspensory ligaments of Cooper, while the intervening skin is swollen due to lymphatic edema [1].
* **Molecular Profile:** IBC is frequently ER/PR negative and often shows HER2/neu overexpression.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 453-454.
Neoplasia Indian Medical PG Question 5: Which mutation is seen in malignant melanoma?
- A. N-MYC
- B. RB gene
- C. CDKN2A (Correct Answer)
- D. p53
Neoplasia Explanation: **Explanation:**
**CDKN2A** (located on chromosome 9p21) is the most frequently mutated gene in both familial and sporadic **Malignant Melanoma** [3]. It is a complex locus that encodes two critical tumor suppressor proteins: **p16/INK4a** (which inhibits CDK4/6, maintaining the RB pathway) and **p14/ARF** (which prevents p53 degradation) [1]. Mutations in CDKN2A lead to uncontrolled cell cycle progression through the G1-S checkpoint [4].
**Analysis of Incorrect Options:**
* **A. N-MYC:** This oncogene is characteristically amplified in **Neuroblastoma** and is a significant prognostic marker (indicates poor prognosis).
* **B. RB Gene:** Located on chromosome 13q14, mutations in the Retinoblastoma (RB) gene are primarily associated with **Retinoblastoma** and **Osteosarcoma**. While the RB *pathway* is affected in melanoma via p16 loss, the primary mutation is in CDKN2A [3].
* **D. p53:** Known as the "Guardian of the Genome," it is the most common mutation in human cancers overall. However, in the specific context of melanoma, CDKN2A and BRAF mutations are more characteristic and diagnostic hallmarks [1].
**High-Yield Clinical Pearls for NEET-PG:**
* **BRAF Mutation:** The most common somatic mutation in sporadic melanoma (specifically **V600E**). It involves the MAPK signaling pathway [1].
* **KIT Mutation:** Commonly seen in mucosal and acral lentiginous melanomas [1].
* **Breslow’s Depth:** The most important prognostic factor for melanoma (measures vertical thickness) [2].
* **S-100 & HMB-45:** Key immunohistochemical (IHC) markers for diagnosis.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Skin, pp. 1150-1151.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Skin, pp. 1152-1153.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 305-306.
[4] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 297-298.
More Neoplasia Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.