Endocrine Pathology Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Endocrine Pathology. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Endocrine Pathology Indian Medical PG Question 1: Which of the following mechanisms is NOT responsible for complications in Diabetes Mellitus?
- A. Non-enzymatic glycosylation
- B. Protein Kinase C activation
- C. Disturbance in polyol pathway
- D. Chronic inflammation (Correct Answer)
Endocrine Pathology Explanation: The pathogenesis of diabetic complications is primarily driven by **hyperglycemia-induced metabolic disturbances** rather than primary chronic inflammation [1]. While diabetes is associated with a low-grade inflammatory state, the specific biochemical pathways leading to microvascular and macrovascular damage are well-defined.
### Why "Chronic Inflammation" is the Correct Answer
Chronic inflammation is a feature of many diseases, but it is **not** considered one of the four primary metabolic pathways (defined by Robbins Pathology) that directly cause diabetic complications. The damage in diabetes is biochemical and structural, resulting from the toxic effects of excess glucose on tissues that do not require insulin for glucose uptake (e.g., nerves, kidneys, blood vessels) [1].
### Explanation of Other Options (The 3 Main Mechanisms)
* **Non-enzymatic glycosylation (Option A):** Glucose binds to proteins (like collagen) without enzymes, forming **Advanced Glycation End-products (AGEs)**. AGEs cross-link proteins, trap LDL in vessel walls, and bind to RAGE (Receptors for AGEs) to release cytokines and pro-coagulant factors [1].
* **Protein Kinase C (PKC) activation (Option B):** Intracellular hyperglycemia increases Diacylglycerol (DAG), which activates PKC [1]. This leads to the production of **VEGF** (causing neovascularization in retinopathy) and **TGF-β** (causing basement membrane thickening).
* **Disturbance in Polyol Pathway (Option C):** In tissues like the lens or nerves, glucose is converted to **sorbitol** by aldose reductase. Sorbitol is osmotically active, leading to water influx, oxidative stress, and depleted glutathione, causing cataracts and peripheral neuropathy.
### NEET-PG High-Yield Pearls
* **The "Fourth" Mechanism:** Not listed here, but often tested, is the **Hexosamine pathway**, which leads to the production of fructose-6-phosphate and contributes to insulin resistance [1].
* **Common Denominator:** All these pathways are triggered by the production of **Reactive Oxygen Species (ROS)** in the mitochondria.
* **HbA1c:** This is a clinical example of non-enzymatic glycosylation used to monitor long-term glycemic control.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1118-1121.
Endocrine Pathology Indian Medical PG Question 2: Pheochromocytoma are tumors of which structure?
- A. Adrenal cortex
- B. Adrenal medulla (Correct Answer)
- C. Pancreas
- D. Bone
Endocrine Pathology Explanation: **Explanation:**
**Pheochromocytoma** is a catecholamine-secreting tumor derived from the **chromaffin cells** [2] of the **adrenal medulla** [3]. These cells are embryologically derived from the **neural crest** and are responsible for synthesizing and secreting epinephrine and norepinephrine [3].
**Analysis of Options:**
* **Adrenal Cortex (Incorrect):** The cortex is derived from the mesoderm and produces steroid hormones (aldosterone, cortisol, and androgens) [3]. Tumors here include Conn’s syndrome or Cushing’s syndrome adenomas.
* **Pancreas (Incorrect):** While the pancreas has endocrine functions (Islets of Langerhans), its tumors (e.g., Insulinoma, Gastrinoma) are distinct from catecholamine-secreting pheochromocytomas.
* **Bone (Incorrect):** Bone is not a site for primary chromaffin cell tumors.
**High-Yield Clinical Pearls for NEET-PG:**
* **The Rule of 10s:** 10% are bilateral, 10% are malignant, 10% occur in children, and 10% are extra-adrenal (known as **Paragangliomas**, most commonly at the Organ of Zuckerkandl) [1].
* **Clinical Triad:** Episodic headache, sweating (diaphoresis), and palpitations/tachycardia, usually accompanied by hypertension [2].
* **Diagnosis:** Best initial screening test is **urinary/plasma metanephrines**.
* **Histology:** Characterized by the **"Zellballen" pattern** (nested clusters of cells surrounded by a vascular stroma) [1].
* **Genetic Associations:** Frequently associated with **MEN 2A and 2B**, von Hippel-Lindau (VHL) syndrome, and Neurofibromatosis type 1 (NF1).
* **Management:** Pre-operative blockade must follow the sequence: **Alpha-blockade first** (e.g., Phenoxybenzamine), followed by Beta-blockade to prevent a hypertensive crisis.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 419-420.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1137-1139.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1125-1126.
Endocrine Pathology Indian Medical PG Question 3: Expression of which of the following oncogenes is associated with a high incidence of medullary carcinoma of the thyroid?
- A. FOS
- B. BRAF
- C. RET Proto oncogene (Correct Answer)
- D. WNT1
Endocrine Pathology Explanation: **Explanation:**
**Medullary Thyroid Carcinoma (MTC)** is a neuroendocrine tumor derived from the parafollicular C-cells [2], which secrete calcitonin. The molecular hallmark of MTC is the mutation of the **RET proto-oncogene**, located on chromosome 10q11.2.
1. **Why RET is correct:**
* **Germline mutations** in RET are responsible for nearly all cases of hereditary MTC, including **MEN 2A, MEN 2B**, and Familial MTC [1].
* **Somatic mutations** in RET are found in approximately 50% of sporadic MTC cases.
* The mutation leads to constitutive activation of the receptor tyrosine kinase, driving uncontrolled cell proliferation.
2. **Why other options are incorrect:**
* **BRAF:** Mutations (specifically V600E) are most commonly associated with **Papillary Thyroid Carcinoma (PTC)** and some Anaplastic carcinomas, not MTC.
* **FOS:** This is an immediate-early gene involved in cell cycle progression but is not a specific diagnostic or prognostic marker for thyroid malignancies.
* **WNT1:** Dysregulation of the Wnt/β-catenin pathway is associated with **Follicular Thyroid Carcinoma** and some variants of Papillary carcinoma (e.g., Cribriform-morular variant), but not MTC.
**High-Yield Clinical Pearls for NEET-PG:**
* **Amyloid Stroma:** Histologically, MTC is characterized by nests of polygonal cells with **amyloid deposits** (derived from pro-calcitonin) that stain with Congo Red.
* **Screening:** In families with known MEN 2 syndromes, prophylactic thyroidectomy is often performed based on the detection of a RET mutation before the cancer even develops [1].
* **Marker:** Serum **Calcitonin** is the primary tumor marker for diagnosis and monitoring recurrence [1].
* **Origin:** C-cells are derived from the **ultimobranchial body** (neural crest origin) [2].
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1102-1103.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 428-429.
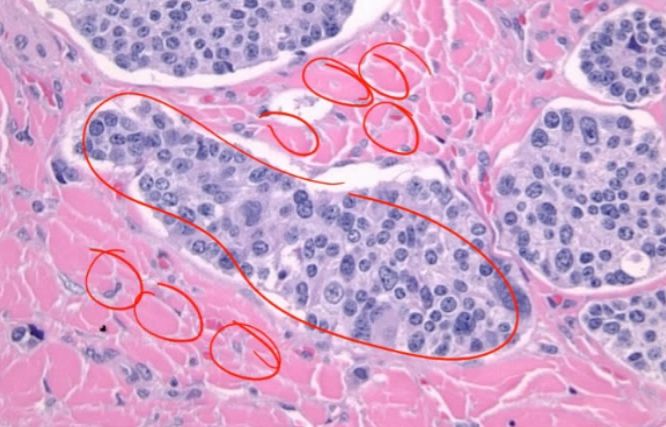
Endocrine Pathology Indian Medical PG Question 4: A biopsy from the parathyroid gland of a 55-year-old male, a known case of chronic kidney disease with hypertension and type II diabetes who recently developed bone pain, skin lesions, and recurrent kidney stones, is shown below. What is the most likely histopathological finding?
- A. Water clear cells in parathyroid hyperplasia (Correct Answer)
- B. Water clear cells in parathyroid carcinoma
- C. Tuberculous parathyroiditis
- D. Parathyroid necrosis
Endocrine Pathology Explanation: ***Water clear cells in parathyroid hyperplasia***
- **Chronic kidney disease** leads to **secondary hyperparathyroidism** due to decreased **vitamin D activation** and **phosphate retention**, causing **parathyroid hyperplasia** with characteristic **water clear cells (wasserhelle cells)**.
- These cells have **abundant clear cytoplasm** due to **glycogen accumulation** and **mitochondrial swelling**, commonly seen in **long-standing hyperparathyroidism** associated with **CKD**.
*Water clear cells in parathyroid carcinoma*
- **Parathyroid carcinoma** would show **capsular invasion**, **vascular invasion**, and **mitotic figures**, which are not typical in **secondary hyperparathyroidism** from CKD.
- **Carcinoma** is extremely rare and usually presents with **severe hypercalcemia** and **rapid onset** symptoms, not the chronic progression seen with CKD.
*Tuberculous parathyroiditis*
- **TB parathyroiditis** would show **caseating granulomas**, **epithelioid cells**, and **Langerhans giant cells**, not water clear cells.
- This condition is extremely rare and would present with **systemic TB symptoms** like **fever**, **weight loss**, and **night sweats**, which are absent here.
*Parathyroid necrosis*
- **Parathyroid necrosis** would show **tissue death**, **inflammatory infiltrate**, and **loss of normal architecture**, not hyperplastic changes.
- This typically occurs in **acute conditions** like **infarction** or **severe hypocalcemia**, not in chronic progressive CKD with bone pain and stones.
Endocrine Pathology Indian Medical PG Question 5: The neuroendocrine carcinoma arising from parafollicular 'C' cells of thyroid is:
- A. Papillary carcinoma
- B. Follicular carcinoma
- C. Medullary carcinoma (Correct Answer)
- D. Anaplastic carcinoma
Endocrine Pathology Explanation: **Explanation:**
**Correct Answer: C. Medullary Carcinoma**
Medullary Thyroid Carcinoma (MTC) is a unique **neuroendocrine tumor** [2] derived from the **parafollicular ‘C’ cells** of the thyroid [1]. Unlike other thyroid cancers, these cells originate from the **neural crest** (ultimobranchial body) rather than the thyroid follicular epithelium. Their primary function is the secretion of **Calcitonin** [1], which serves as a crucial tumor marker for diagnosis and monitoring recurrence [3].
**Analysis of Incorrect Options:**
* **A. Papillary Carcinoma:** The most common thyroid malignancy; it arises from follicular cells and is characterized by nuclear features like Orphan Annie eye nuclei and Psammoma bodies.
* **B. Follicular Carcinoma:** Arises from follicular cells; it is characterized by capsular or vascular invasion [2] and typically spreads hematogenously [1].
* **D. Anaplastic Carcinoma:** A highly aggressive, undifferentiated tumor arising from follicular cells [2], usually seen in elderly patients.
**High-Yield NEET-PG Pearls:**
* **Histology:** Shows nests of polygonal cells in an **amyloid stroma** (formed by altered calcitonin) [2]. Amyloid stains positive with **Congo Red** (apple-green birefringence).
* **Genetics:** Approximately 20-25% are familial, associated with **MEN 2A and 2B** syndromes [1] involving **RET proto-oncogene** mutations.
* **Staining:** Positive for neuroendocrine markers like **Chromogranin A**, Synaptophysin, and Calcitonin.
* **Prophylaxis:** In patients with known RET mutations, prophylactic thyroidectomy is often indicated.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 428-429.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 430-431.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1102-1103.
More Endocrine Pathology Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.