

Intro to Endocrine Testing - Hormonal Hullabaloo
- Assays: RIA, ELISA, Chemiluminescence (CLIA).
- Specimens: Critical timing (circadian/pulsatile rhythms), stability, specific anticoagulants (e.g., EDTA for PTH).
- Pre-analytical factors: Stress, posture (e.g., renin), medications can alter hormone levels.
- Secretion patterns: Pulsatile (e.g., LH, GH), Circadian (e.g., cortisol, ACTH), Feedback loops (mostly negative).
- Testing types:
- Static: Basal hormone levels (e.g., TSH, HbA1c).
- Dynamic: Stimulation (e.g., ACTH for adrenal reserve) or Suppression (e.g., Dexamethasone for Cushing's).
⭐ Hook effect in immunoassays: Very high antigen levels (e.g., prolactin in prolactinoma) can cause falsely low readings. Overcome by sample dilution.
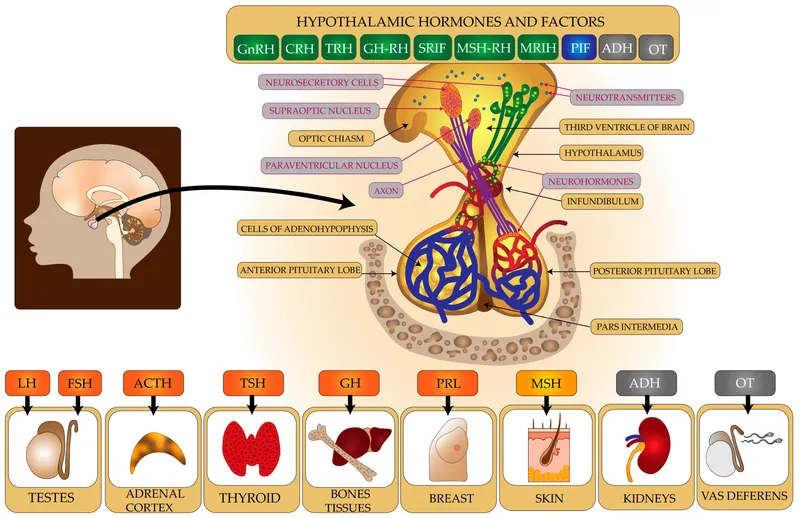
Hypothalamic-Pituitary Tests - Master Gland Metrics
- Growth Hormone (GH):
- Screen: IGF-1 (more stable).
- Acromegaly/Gigantism: Oral Glucose Tolerance Test (OGTT) - GH fails to suppress <1 ng/mL.
- Deficiency: Insulin Tolerance Test (ITT) is gold standard; GH stimulation tests (e.g., Arginine, Clonidine).
- Prolactin (PRL):
- Basal PRL: >200 ng/mL highly suggestive of prolactinoma.
- Dynamic tests (e.g., TRH stimulation) less common; screen for macroprolactin if indicated.
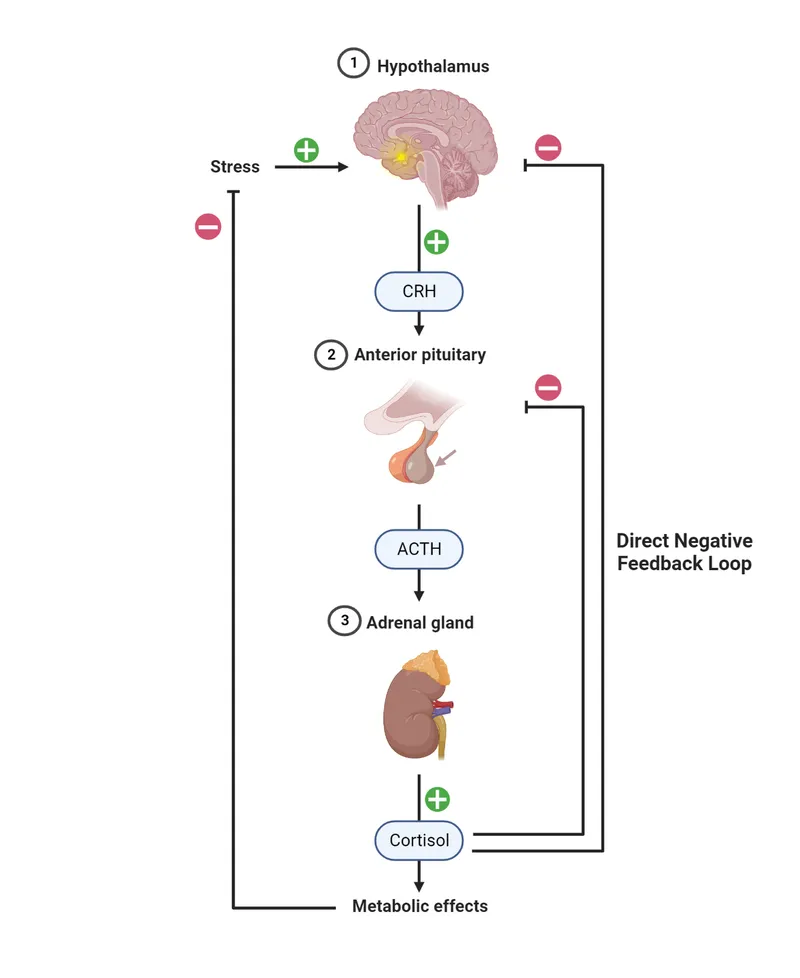
- ACTH (Cushing's Syndrome Workup):
- Basal: Morning ACTH & Cortisol.
- Low-Dose Dexamethasone Suppression Test (LDDST - 1mg overnight): Failure to suppress cortisol suggests Cushing's Syndrome.
- High-Dose Dexamethasone Suppression Test (HDDST - 8mg overnight): Cortisol suppression → Cushing's Disease (pituitary); No suppression → Ectopic ACTH / Adrenal tumor.
- CRH Stimulation Test: Exaggerated ACTH/cortisol response in Cushing's Disease.
- TSH: Assessed with free T4 (FT4) & T3 as part of thyroid function tests.
- ADH (Vasopressin) - Diabetes Insipidus (DI):
- Water Deprivation Test: Differentiates Central DI (Urine Osm ↑ >50% post-DDAVP) from Nephrogenic DI (minimal/no Urine Osm ↑ post-DDAVP).
⭐ Paradoxical GH rise with TRH or GnRH stimulation occurs in approximately 50% of patients with acromegaly.
Thyroid & Parathyroid Tests - Neck Check Diagnostics
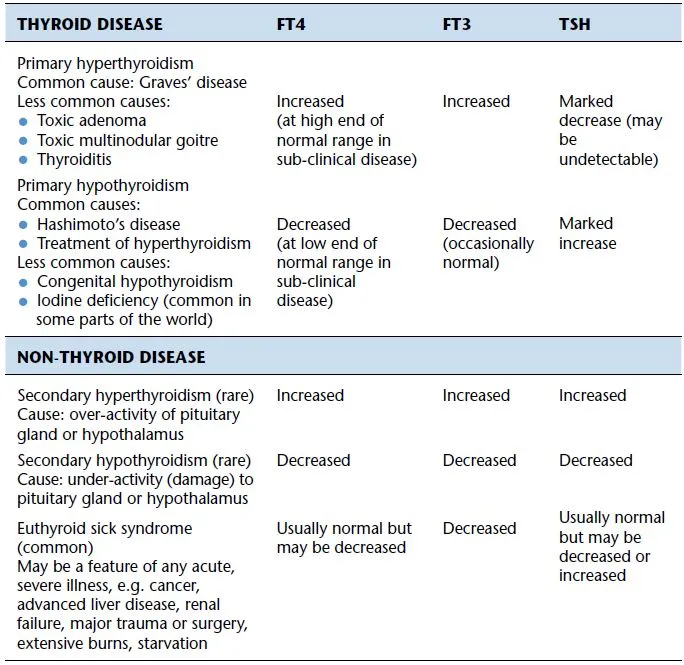
- Thyroid Function Tests (TFTs):
- TSH: 0.4-4.0 mIU/L. Best initial. ↑Primary Hypo, ↓Primary Hyper.
- fT4: 0.8-1.8 ng/dL; fT3: 2.3-4.2 pg/mL (more potent).
- Antibodies: TPOAb/TgAb (Hashimoto’s), TRAb (Graves’).
- Subclinical Hypo: ↑TSH, Normal fT4. Subclinical Hyper: ↓TSH, Normal fT4/fT3.
- Non-Thyroidal Illness (NTI): ↓T3, ↓/Normal T4, Normal/↓ TSH.
- Parathyroid Tests:
- PTH, Serum Ca (Total: 8.5-10.5 mg/dL; Ionized: 4.65-5.25 mg/dL), Phosphate (2.5-4.5 mg/dL), Vit D (25-OH, 1,25-(OH)2).
- Corrected Ca: $Ca_{corr} (mg/dL) = Ca_{total} (mg/dL) + 0.8 \times (4.0 - Albumin [g/dL])$.
- Primary Hyperparathyroidism: ↑PTH, ↑Ca, ↓PO4.
- Hypoparathyroidism: ↓PTH, ↓Ca, ↑PO4.
⭐ TSH is the single most sensitive test for primary thyroid dysfunction.
Adrenal & Pancreatic Tests - Stress & Sugar Sleuthing
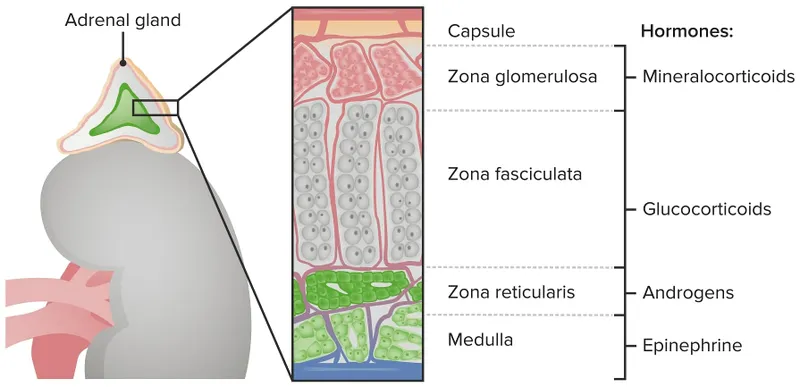
- Adrenal Tests:
- Cortisol: Serum, 24hr urine free cortisol (UFC), late-night salivary.
- ACTH: Basal, stimulated.
- Dexamethasone Suppression Test (DST):
- Low Dose (LDDST): 1mg overnight; failure to suppress cortisol → Cushing's syndrome.
- High Dose (HDDST): 8mg; differentiates pituitary vs. ectopic ACTH.
- CRH Stimulation: Differentiates Cushing's disease from ectopic ACTH.
- Aldosterone & Renin: For hyperaldosteronism (ARR).
- Metanephrines (plasma/urine), VMA (urine): For pheochromocytoma.
- 📌 Mnemonic (Adrenal Cortex): GFR - Salt (Glomerulosa-Aldosterone), Sugar (Fasciculata-Cortisol), Sex (Reticularis-Androgens).
- Pancreatic Endocrine Tests:
- Glucose: Fasting (FPG), Post-prandial (PPG), Random.
- Diabetes: FPG ≥ 126 mg/dL; PPG (OGTT) ≥ 200 mg/dL.
- HbA1c: Glycated hemoglobin.
- Diabetes: ≥ 6.5%.
- Oral Glucose Tolerance Test (OGTT): 75g glucose load.
- Insulin, C-peptide: Assess insulin secretion/resistance.
- Glucose: Fasting (FPG), Post-prandial (PPG), Random.
⭐ HbA1c reflects glycemic control over the preceding 2-3 months.
High‑Yield Points - ⚡ Biggest Takeaways
- Basal hormone levels screen; dynamic tests (stimulation/suppression) confirm dysfunction (e.g., Cushing's, Addison's).
- Immunoassays (ELISA, RIA) are pivotal for quantifying most hormone concentrations.
- Urinary Free Cortisol (UFC) and metanephrines/VMA are crucial for Cushing's syndrome and pheochromocytoma.
- Autoantibodies (anti-TPO, anti-TSHR, anti-GAD) diagnose autoimmune thyroiditis and Type 1 DM.
- HbA1c reflects long-term glycemic control (2-3 months) in diabetes.
- FNAC is the primary diagnostic tool for thyroid nodules.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more