
Arterial pressure waveform — MCQs

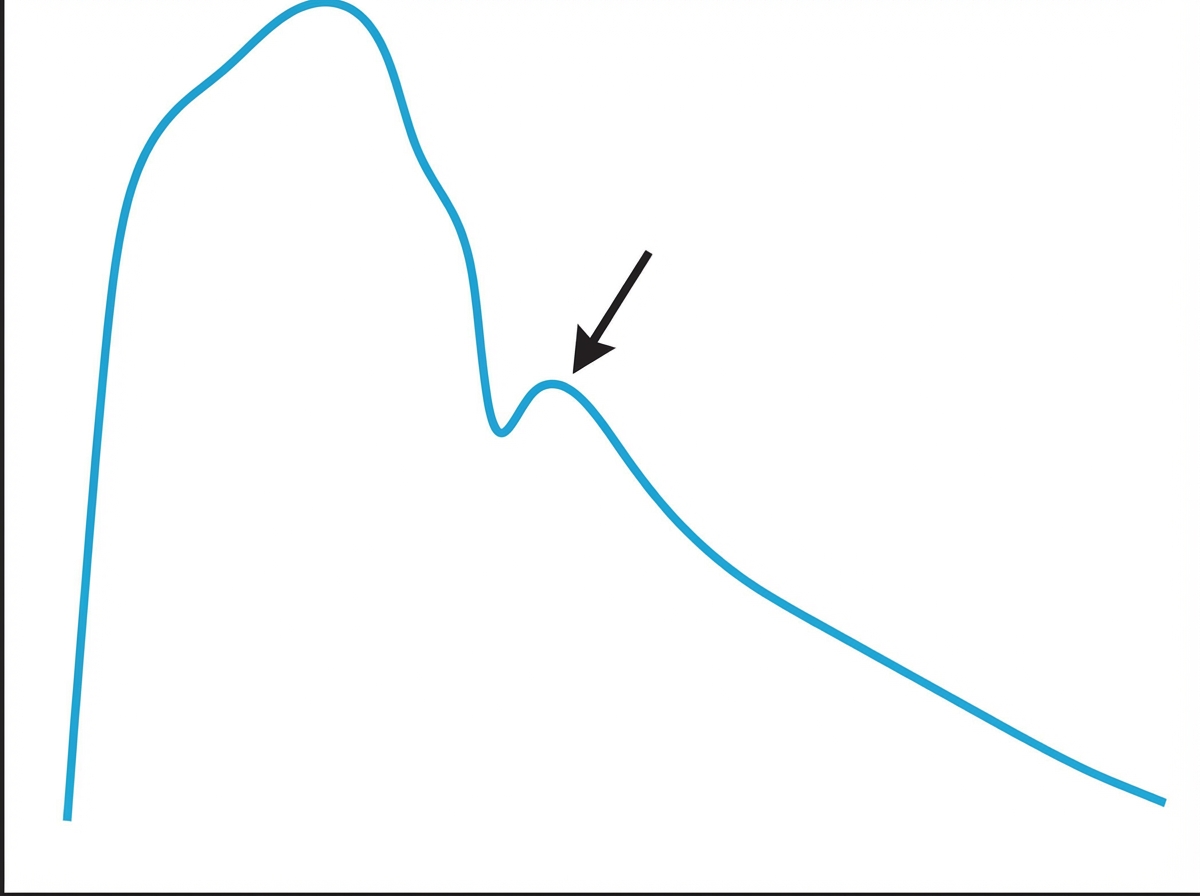
Prior to undergoing a total knee arthroplasty, a 62-year-old man with coronary artery disease undergoes diagnostic cardiac catheterization. The catheter is inserted via the femoral artery and then advanced to the ascending aorta. Pressure tracing of the catheter is shown. The peak marked by the arrow is most likely caused by which of the following?
A 32-year-old woman comes to the office for a regular follow-up. She was diagnosed with type 2 diabetes mellitus 4 years ago. Her last blood test showed a fasting blood glucose level of 6.6 mmol/L (118.9 mg/dL) and HbA1c of 5.1%. No other significant past medical history. Current medications are metformin and a daily multivitamin. No significant family history. The physician wants to take her blood pressure measurements, but the patient states that she measures it every day in the morning and in the evening and even shows him a blood pressure diary with all the measurements being within normal limits. Which of the following statements is correct?
A 27-year-old male arrives in the emergency department with a stab wound over the precordial chest wall. The patient is in distress and is cold, sweaty, and pale. Initial physical examination is significant for muffled heart sounds, distended neck veins, and a 3 cm stab wound near the left sternal border. Breath sounds are present bilaterally without evidence of tracheal deviation. Which of the following additional findings would be expected on further evaluation?
A 17-year-old previously healthy, athletic male suddenly falls unconscious while playing soccer. His athletic trainer comes to his aid and notes that he is pulseless. He begins performing CPR on the patient until the ambulance arrives but the teenager is pronounced dead when the paramedics arrived. Upon investigation of his primary care physician's office notes, it was found that the child had a recognized murmur that was ruled to be "benign." Which of the following conditions would have increased the intensity of the murmur?
An experiment to determine the effects of gravity on blood pressure is conducted on 3 individuals of equal height and blood pressure oriented in different positions in space. Participant A is strapped in a supine position on a bed turned upside down in a vertical orientation with his head towards the floor and his feet towards the ceiling. Participant B is strapped in a supine position on a bed turned downwards in a vertical orientation with his head towards the ceiling and his feet just about touching the floor. Participant C is strapped in a supine position on a bed in a horizontal orientation. Blood pressure readings are then taken at the level of the head, heart, and feet from all 3 participants. Which of these positions will have the lowest recorded blood pressure reading?
An 83-year-old male presents with dyspnea, orthopnea, and a chest radiograph demonstrating pulmonary edema. A diagnosis of congestive heart failure is considered. The following clinical measurements are obtained: 100 bpm heart rate, 0.2 mL O2/mL systemic blood arterial oxygen content, 0.1 mL O2/mL pulmonary arterial oxygen content, and 400 mL O2/min oxygen consumption. Using the above information, which of the following values represents this patient's cardiac stroke volume?
A 60-year-old male engineer who complains of shortness of breath when walking a few blocks undergoes a cardiac stress test because of concern for coronary artery disease. During the test he asks his cardiologist about what variables are usually used to quantify the functioning of the heart. He learns that one of these variables is stroke volume. Which of the following scenarios would be most likely to lead to a decrease in stroke volume?
A 27-year-old man is running on the treadmill at his gym. His blood pressure prior to beginning his workout was 110/72. Which of the following changes in his cardiovascular system may be seen in this man now that he is exercising?
A 34-year-old male is brought to the emergency department. He has prior hospitalizations for opiate overdoses, but today presents with fever, chills, rigors and malaise. On physical exam vitals are temperature: 100.5 deg F (38.1 deg C), pulse is 105/min, blood pressure is 135/60 mmHg, and respirations are 22/min. You note the following findings on the patient's hands (Figures A and B). You note that as the patient is seated, his head bobs with each successive heart beat. Which of the following findings is most likely present in this patient?

A 3-year-old boy is brought to the physician because of recurrent nosebleeds and fatigue for the past 2 months. He also frequently complains his head hurts. The patient has met all motoric milestones for his age but does not like to run because his legs start to hurt if he does. He is at the 40th percentile for both height and weight. His temperature is 37.0°C (98.6°F), pulse is 125/min, respirations are 32/min, and blood pressure in the right arm is 130/85 mm Hg. A grade 2/6 systolic murmur is heard in the left paravertebral region. Further evaluation of this patient is most likely to show which of the following findings?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app