
Cholinergic/Adrenergic drugs — MCQs

On this page
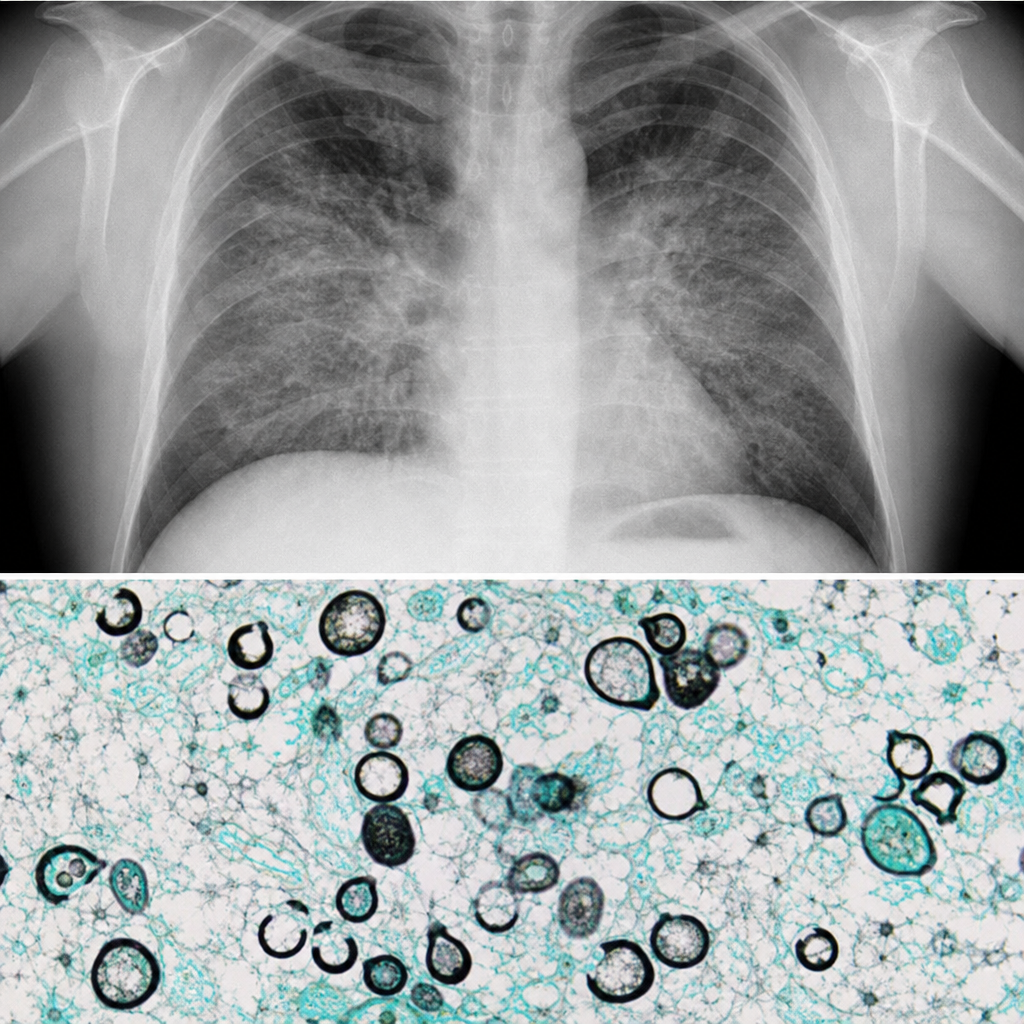
A 45-year-old man with a renal transplant performed 18 months ago has been maintained on tacrolimus, mycophenolate mofetil, and prednisone. He now presents with a three-week history of progressive dyspnea and non-productive cough. Chest radiograph shows bilateral perihilar interstitial infiltrates. Bronchoalveolar lavage reveals disc-shaped organisms with a characteristic morphology on Grocott-Gomori methenamine silver stain. The infectious disease team recommends trimethoprim-sulfamethoxazole as first-line therapy. Which of the following best describes the key host defense that is impaired in this patient, making him susceptible to this infection?
A chronic smoker wants to quit smoking. Which of the following is the MOST appropriate first-line pharmacotherapy for smoking cessation?
A mother reports that her daughter ingested a substance in an unknown dose. The girl presents with hypertension, tachycardia, mydriasis, and hyperthermia. What is the most likely substance?
A 30-year-old drug addict presents to the emergency department with signs of unknown drug poisoning. The patient exhibits dilated pupils, diaphoresis, tachycardia, and tremors. On examination, the blood pressure is 180/110 mmHg, and the heart rate is 120 beats per minute. What is the most likely diagnosis?
A 45-year-old patient with a history of depression was initially being treated with sertraline, but his symptoms were not adequately controlled. His medication regimen was changed to include an MAO inhibitor and amitriptyline. Shortly after the change in medication, the patient developed agitation, seizures, hyperreflexia, and tremor. Which of the following is the most appropriate treatment for this patient?
Practice by Chapter
Acetylcholine receptors and function
Practice Questions
Cholinergic agonists (direct and indirect)
Practice Questions
Muscarinic antagonists
Practice Questions
Nicotinic antagonists
Practice Questions
Neuromuscular blocking agents
Practice Questions
Adrenergic receptor subtypes
Practice Questions
Alpha-adrenergic agonists
Practice Questions
Beta-adrenergic agonists
Practice Questions
Alpha-adrenergic antagonists
Practice Questions
Beta-adrenergic antagonists
Practice Questions
Sympathomimetics
Practice Questions
Autonomic drug interactions
Practice Questions
Clinical applications in autonomic disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app