
Antibiotics — MCQs

On this page
A 57-year-old woman is brought to the emergency department because of crampy abdominal pain and foul-smelling, watery diarrhea. One week ago, she underwent treatment of cellulitis with clindamycin. She has developed shortness of breath and urticaria after treatment with vancomycin in the past. Her temperature is 38.4°C (101.1°F). Abdominal examination shows mild tenderness in the left lower quadrant. Her leukocyte count is 12,800/mm3. An enzyme immunoassay is positive for glutamate dehydrogenase antigen and toxins A and B. Which of the following is the mechanism of action of the most appropriate pharmacotherapy for this patient's condition?
A 40-year-old man comes to the physician because of a 6-week history of increasing shortness of breath, fatigue, and fever. He has had a cough productive of foul-smelling sputum for 4 weeks. He was hospitalized for alcohol intoxication twice over the past 6 months. He has hypertension and depression. He has smoked one pack of cigarettes daily for 20 years and drinks 6 alcoholic beverages daily. Current medications include ramipril and fluoxetine. He appears malnourished. He is 185 cm (6 ft 1 in) tall and weighs 65.7 kg (145 lb); BMI is 19.1 kg/m2. His temperature is 38.3°C (100.9°F), pulse is 118/min, respirations are 24/min, and blood pressure is 147/96 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 94%. Examination of the chest shows dullness to percussion over the right upper lung field. An x-ray of the chest shows a lung cavity with an air-fluid level and surrounding infiltrate in the right upper lobe of the lung. Which of the following is the most appropriate next step in management?
A 15-year-old boy presents with his father to the urgent care with 5 days of frequent diarrhea, occasionally with streaks of blood mixed in. Stool cultures are pending, but preliminary stool samples demonstrate fecal leukocytes and erythrocytes. His vital signs are as follows: blood pressure is 126/83 mm Hg, heart rate is 97/min, and respiratory rate is 15/min. He is started on outpatient therapy for presumed Shigella infection. Which of the following is the most appropriate therapy?
A 22-year-old man presents to a physician with a single painless ulcer on his glans penis that he first noticed 2 weeks ago. He mentions that he is sexually active with multiple partners. There is no history of fevers. Initially, he thought that the ulcer would go away on its own, but decided to come to the clinic because the ulcer persisted. On palpation of the ulcer, the edge and base are indurated. There is no purulence. Multiple painless, firm, and non-fixed lymph nodes are present in the inguinal regions bilaterally. The physician orders a Venereal Disease Research Laboratory (VDRL) test, which is positive. The Treponema pallidum particle agglutination assay is also positive. Upon discussing the diagnosis, the patient informs the physician that he has a severe allergy to penicillin and he declines treatment with an injectable medicine. Which of the following drugs is most appropriate for this patient?
A 31-year-old woman, gravida 1, para 0, at 10 weeks' gestation comes to the physician because of a rash on her upper arm that appeared 3 days ago. She has also had headaches and muscle aches for 1 day. She went on a camping trip in Maine 10 days ago. Her temperature is 39°C (102.2°F). A photograph of her rash is shown. Which of the following is the most appropriate pharmacotherapy?

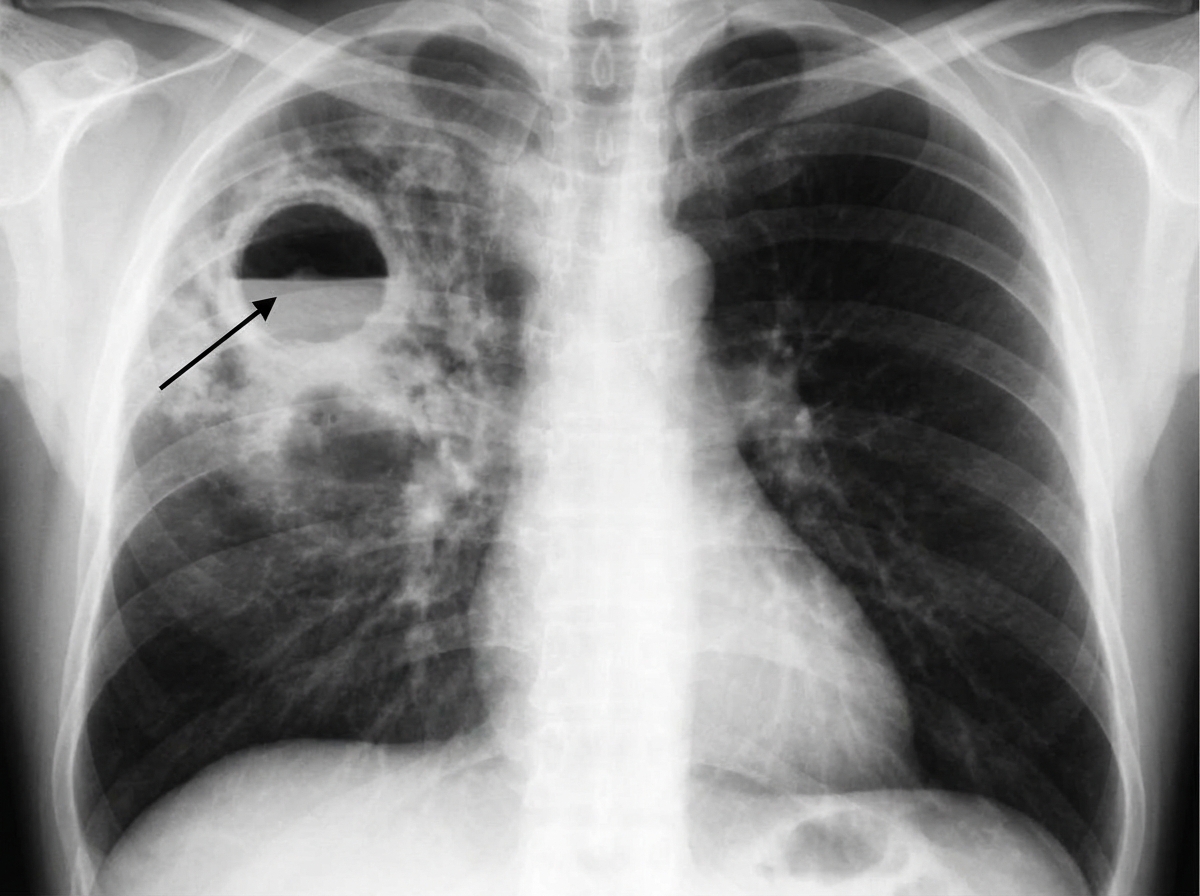
A 61-year-old woman who recently emigrated from India comes to the physician because of a 2-month history of fever, fatigue, night sweats, and a productive cough. She has had a 5-kg (11-lb) weight loss during this period. She has a history of type 2 diabetes mellitus and poorly controlled asthma. She has had multiple asthma exacerbations in the past year that were treated with glucocorticoids. An x-ray of the chest shows a cavitary lesion of the posterior apical segment of the left upper lobe with consolidation of the surrounding parenchyma. The pathogen identified on sputum culture is found to be resistant to multiple drugs, including streptomycin. Which of the following mechanisms is most likely involved in bacterial resistance to this drug?
A 35-year-old woman visits the office with complaints of yellowish vaginal discharge and increased urinary frequency for a week. She also complains of pain during urination. Past medical history is irrelevant. She admits to having multiple sexual partners in the past few months. Physical examination is within normal limits except for lower abdominal tenderness. Urine culture yields Chlamydia trachomatis. What is the most appropriate next step in the management of this patient?
A 30-year-old woman with HIV comes to the emergency department because of fever and multiple skin lesions for 1 week. She also has nausea, anorexia, and abdominal pain. The skin lesions are non-pruritic and painless. She has smoked one pack of cigarettes daily for 15 years and drinks 2 beers daily. She has been using intravenous crack cocaine for 6 years. She appears ill. Her temperature is 38°C (100.4°F), pulse is 105/min, blood pressure is 110/75 mm Hg. Her BMI is 19 kg/m2. Examination shows track marks on both cubital fossae. There are white patches on her palate that can be scraped off. There are several red papules measuring 1 to 2 cm on her face and trunk. Her CD4+T-lymphocyte count is 98/mm3 (N ≥ 500). Biopsy of a skin lesion shows vascular proliferation and small black bacteria on Warthin-Starry stain. Which of the following is the most appropriate pharmacotherapy?
You are treating a neonate with meningitis using ampicillin and a second antibiotic, X, that is known to cause ototoxicity. What is the mechanism of antibiotic X?
A 22-year-old female presents to an urgent care clinic for evaluation of a loose bowel movement that she developed after returning from her honeymoon in Mexico last week. She states that she has been having watery stools for the past 3 days at least 3 times per day. She now has abdominal cramps as well. She has no significant past medical history, and the only medication she takes is depot-medroxyprogesterone acetate. Her blood pressure is 104/72 mm Hg; heart rate is 104/min; respiration rate is 14/min, and temperature is 39.4°C (103.0°F). Her physical examination is normal aside from mild diffuse abdominal tenderness and dry mucous membranes. Stool examination reveals no ova. Fecal leukocytes are not present. A stool culture is pending. In addition to oral rehydration, which of the following is the best treatment option for this patient?
Practice by Chapter
Penicillins and beta-lactamase inhibitors
Practice Questions
Cephalosporins
Practice Questions
Carbapenems and monobactams
Practice Questions
Fluoroquinolones
Practice Questions
Aminoglycosides
Practice Questions
Macrolides, ketolides, and lincosamides
Practice Questions
Tetracyclines and glycylcyclines
Practice Questions
Sulfonamides and trimethoprim
Practice Questions
Vancomycin and other glycopeptides
Practice Questions
Oxazolidinones and streptogramins
Practice Questions
Daptomycin and lipopeptides
Practice Questions
Polymyxins
Practice Questions
Antibiotic resistance mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app