
Antibiotics — MCQs

On this page
A 26-year-old woman comes to the emergency department 30 minutes after she was bitten by her neighbor's cat. She has no history of serious illness and takes no medications. She received all recommended immunizations during childhood but has not received any since then. Vital signs are within normal limits. Physical examination shows four puncture wounds on the thenar eminence of the right hand. There is mild swelling but no erythema. There is normal range of motion of her right thumb and wrist. The wound is cleaned with povidone iodine and irrigated with saline. Which of the following is the most appropriate next step in management?
A 13-year-old male is admitted to the hospital for treatment of acute lymphoblastic leukemia. During his hospital course, he develops a fever of 39.0 degrees Celsius. A CBC demonstrates a leukocyte count of <500 /mm^3. Which of the following is the most appropriate initial management of this patient?
A 22-year-old female with no past medical history presents to her primary care physician with a 3-day history of knee pain. She denies any recent injury or trauma. On physical examination her knee is warm, erythematous, and has diminished range of movement. The patient reports having multiple sexual partners over the last year and does not use protection regularly. Her blood pressure is 124/85 mmHg, heart rate is 76/min, and temperature is 38.3℃ (101.0℉). A joint aspiration is performed and a growth of gram-negative diplococci is noted on bacterial culture. What is the treatment of choice for this patient's condition?
A 61-year-old woman is brought to the emergency department because of fever, chills, and flank pain for 8 hours. Her temperature is 39.1°C (102.4°F). Physical examination shows right costovertebral angle tenderness. Urine dipstick is positive for nitrites. Urinalysis shows gram-negative rods. The patient is admitted to the hospital and treatment with a drug that directly inhibits bacterial DNA replication is begun. This drug inhibits a protein that is normally responsible for which of the following steps of DNA replication?
A 54-year-old man presents with fever, abdominal pain, nausea, and bloody diarrhea. He says that his symptoms started 36 hours ago and have not improved. Past medical history is significant for a left-leg abscess secondary to an injury he sustained from a fall 4 days ago while walking his dog. He has been taking clindamycin for this infection. In addition, he has long-standing gastroesophageal reflux disease, managed with omeprazole. His vital signs include: temperature 38.5°C (101.3°F), respiratory rate 19/min, heart rate 90/min, and blood pressure 110/70 mm Hg. Which of the following is the best course of treatment for this patient’s most likely diagnosis?
An investigator is studying the chemical structure of antibiotics and its effect on bacterial growth. He has synthesized a simple beta-lactam antibiotic and has added a bulky side chain to the molecule that inhibits the access of bacterial enzymes to the beta-lactam ring. The synthesized drug will most likely be appropriate for the treatment of which of the following conditions?
A 49-year-old woman comes to the physician because of a 4-month history of fatigue and recurrent pain in both of her wrists and her fingers. During this time, she has also had stiffness of her joints for about 80 minutes after waking up in the morning. Examination shows swelling and tenderness of the wrists and metacarpophalangeal joints bilaterally. Her serum erythrocyte sedimentation rate is 42 mm/h and rheumatoid factor is positive. Treatment is begun with a drug that results in decreased synthesis of deoxythymidine monophosphate. This mechanism is most similar to the mechanism of action of which of the following drugs?
A 7-year-old girl is brought by her parents to her pediatrician's office for a persistent cough observed over the past month. She was diagnosed with cystic fibrosis 2 years ago and has been receiving chest physiotherapy regularly and the flu vaccine yearly. Her parents tell the pediatrician that their daughter has been coughing day and night for the past month, and produces thick, purulent, foul-smelling sputum. They are concerned because this is the first time such an episode has occurred. She has not had a fever, chills or any other flu-like symptoms. On examination, her blood pressure is 100/60 mm Hg, the pulse is 82/min, and the respiratory rate is 16/min. Breath sounds are reduced over the lower lung fields along with a presence of expiratory wheezing. Her sputum culture comes back positive for an aerobic, non-lactose fermenting, oxidase-positive, gram-negative bacillus. Which of the following prophylactic regimes should be considered after treating this patient for her current symptoms?
A 42-year-old man with chronic hepatitis C is admitted to the hospital because of jaundice and abdominal distention. He is diagnosed with decompensated liver cirrhosis, and treatment with diuretics is begun. Two days after admission, he develops abdominal pain and fever. Physical examination shows tense ascites and diffuse abdominal tenderness. Paracentesis yields cloudy fluid with elevated polymorphonuclear (PMN) leukocyte count. A drug with which of the following mechanisms is most appropriate for this patient's condition?
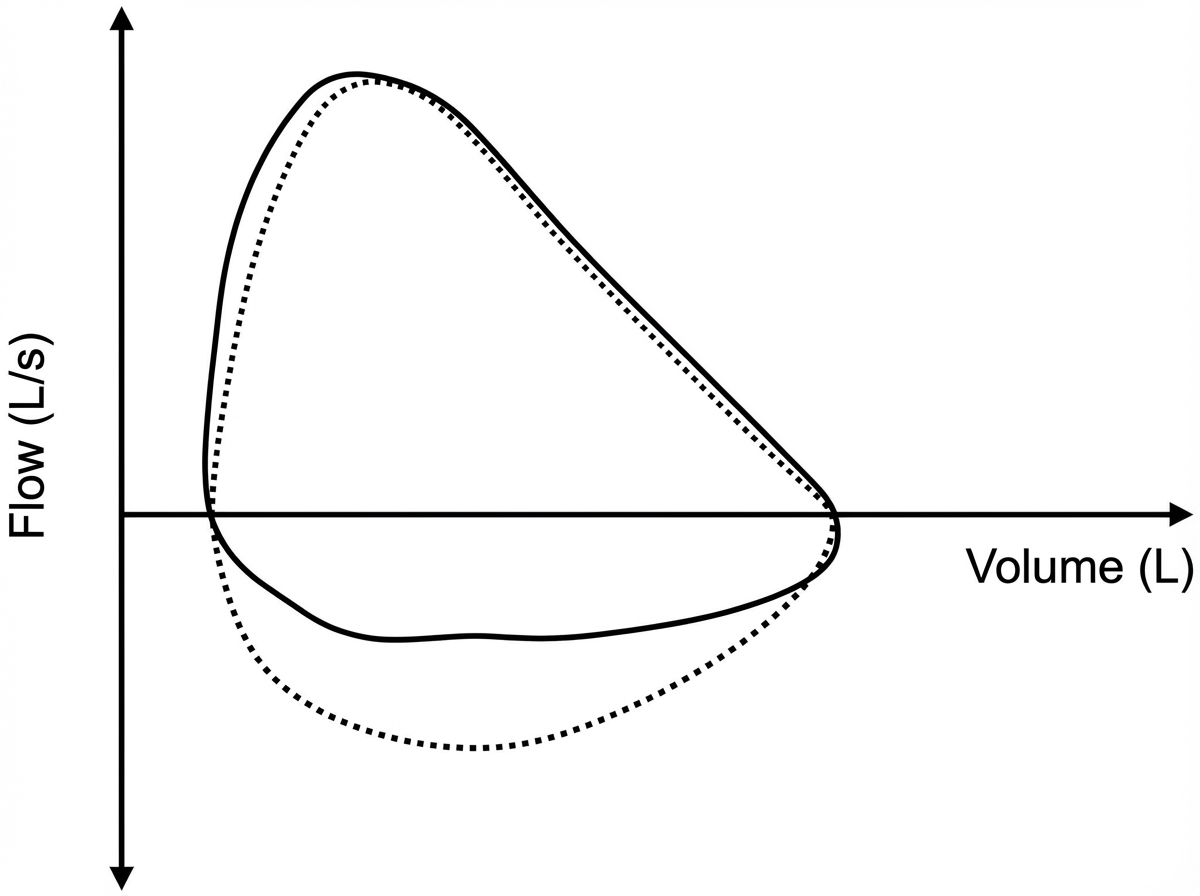
Five minutes after arriving in the postoperative care unit following total knee replacement under general anesthesia, a 55-year-old woman is acutely short of breath. The procedure was uncomplicated. Postoperatively, prophylactic treatment with cefazolin was begun and the patient received morphine and ketorolac for pain management. She has generalized anxiety disorder. Her only other medication is escitalopram. She has smoked one pack of cigarettes daily for 25 years. Her temperature is 37°C (98.6°F), pulse is 108/min, respirations are 26/min, and blood pressure is 95/52 mm Hg. A flow-volume loop obtained via bedside ventilator monitoring is shown; the solid line represents the patient's tracing and the dotted line represents the predicted normal tracing. Which of the following is the most likely underlying cause of this patient's symptoms?
Practice by Chapter
Penicillins and beta-lactamase inhibitors
Practice Questions
Cephalosporins
Practice Questions
Carbapenems and monobactams
Practice Questions
Fluoroquinolones
Practice Questions
Aminoglycosides
Practice Questions
Macrolides, ketolides, and lincosamides
Practice Questions
Tetracyclines and glycylcyclines
Practice Questions
Sulfonamides and trimethoprim
Practice Questions
Vancomycin and other glycopeptides
Practice Questions
Oxazolidinones and streptogramins
Practice Questions
Daptomycin and lipopeptides
Practice Questions
Polymyxins
Practice Questions
Antibiotic resistance mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app