
Antibiotics — MCQs

On this page
Three days after admission to the hospital following a motor vehicle accident, a 45-year-old woman develops a fever. A central venous catheter was placed on the day of admission for treatment of severe hypotension. Her temperature is 39.2°C (102.5°F). Examination shows erythema surrounding the catheter insertion site at the right internal jugular vein. Blood cultures show gram-positive, catalase-positive cocci that have a high minimum inhibitory concentration when exposed to novobiocin. Which of the following is the most appropriate pharmacotherapy?
A 77-year-old woman is brought to the emergency department from her nursing home because she was found down overnight. On presentation she was found to be delirious and was unable to answer questions. Chart review shows that she is allergic to cephalosporins. Her temperature is 102.2°F (39°C), blood pressure is 105/52 mmHg, pulse is 94/min, and respirations are 23/min. Physical exam reveals a productive cough. A metabolic panel is obtained with the following results: Serum: Na+: 135 mEq/L Cl-: 95 mEq/L K+: 4 mEq/L HCO3-: 19 mEq/L BUN: 40 mg/dL Creatinine: 2.5 mg/dL Glucose: 150 mg/dL Based on these findings two different drugs are started empirically. Gram stain on a blood sample is performed showing the presence of gram-positive organisms on all samples. One of the drugs is subsequently stopped. The drug that was most likely stopped has which of the following characteristics?
A 68-year-old man comes to the physician because of headache, fatigue, and nonproductive cough for 1 week. He appears pale. Pulmonary examination shows no abnormalities. Laboratory studies show a hemoglobin concentration of 9.5 g/dL and an elevated serum lactate dehydrogenase concentration. A peripheral blood smear shows normal red blood cells that are clumped together. Results of cold agglutinin titer testing show a 4-fold elevation above normal. An x-ray of the chest shows diffuse, patchy infiltrates bilaterally. Treatment is begun with an antibiotic that is also used to promote gut motility. Which of the following is the primary mechanism of action of this drug?
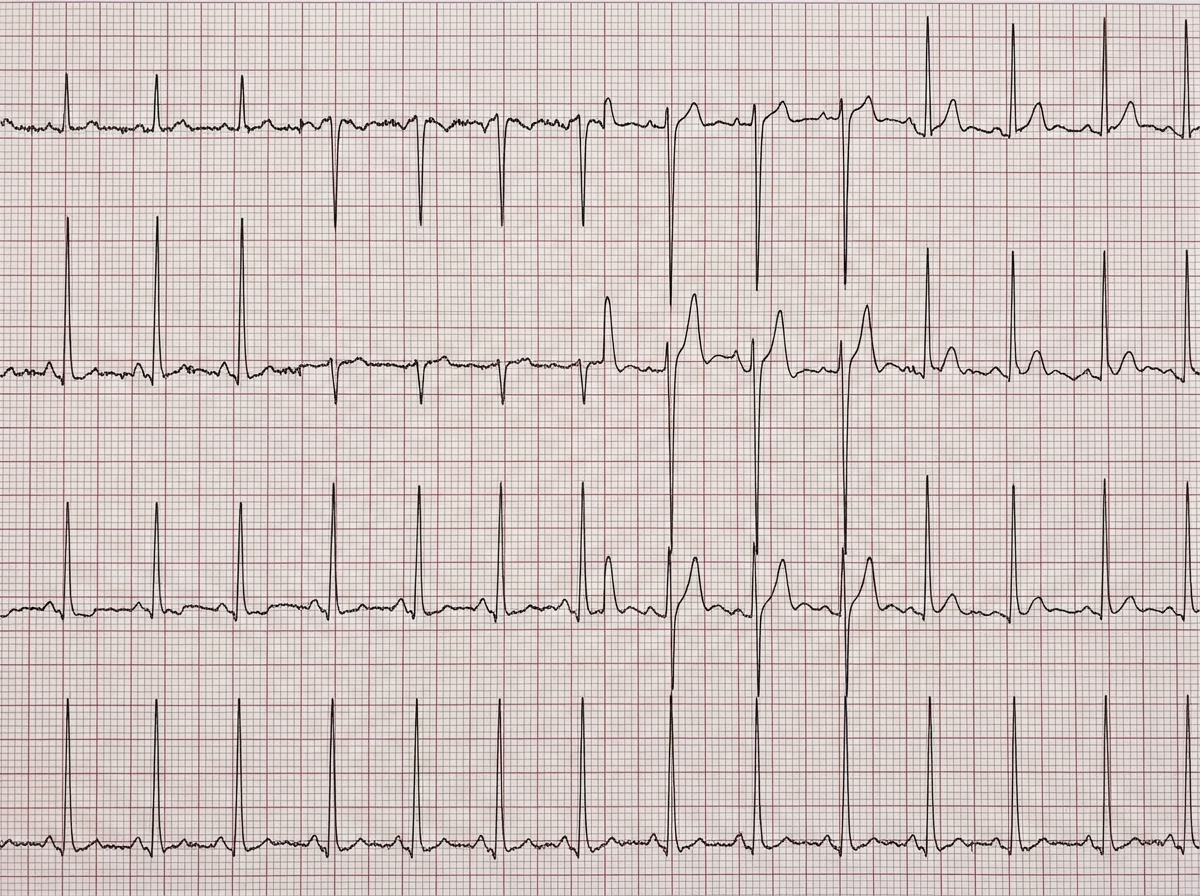
A 24-year-old woman comes to the emergency department because she has had dyspnea and palpitations occurring with mild exertion for the past 8 days. At first, the symptoms subsided immediately after cessation of activity, but they have become worse and now last up to 45 minutes. The patient returned from a summer camping trip in Vermont 6 weeks ago. Except for an episode of flu with fever and chills a month ago, she has no history of serious illness. Her father had a myocardial infarction at the age of 56. She drinks two to four beers on social occasions and occasionally smokes marijuana. Her temperature is 37°C (98.6°F), pulse is 47/min, respirations are 20/min, and blood pressure is 150/70 mm Hg. A resting ECG is shown. Two-step serological testing confirms the diagnosis. Which of the following is the most appropriate next step in management?
A 49-year-old man presents to the clinic for evaluation of puncture wounds on the dorsal aspect of his right second and third metacarpals. He states that he was in a fight 3 nights ago and he struck another individual in the mouth. The patient’s medical history is significant for peripheral vascular disease and hypertension. He takes aspirin, sulfasalazine, and lisinopril. He is allergic to penicillin. He drinks socially on weekends and smokes one and one-half packs of cigarettes daily. Vitals of the patient are as follows: blood pressure is 142/88 mm Hg; heart rate is 88/min; respiratory rate is 14/min; temperature is 38.9°C (102.1°F). On physical examination, the patient appears alert and oriented. His BMI is 33 kg/ m². His eyes are without scleral icterus. His right orbital region reveals ecchymosis along the superior and inferior borders. His heart is regular in rhythm and rate without murmurs. Capillary refill is 4 seconds in fingers and toes. His right dorsal second and third metacarpal region reveals two 3 mm lacerations with edema. Which of the following is the most appropriate management strategy for this patient?
A 29-year-old woman presents to the emergency department with a history of a fever that "won't break." She has taken acetaminophen without relief. Upon obtaining a past medical history you learn that the patient is a prostitute who is homeless with a significant history of intravenous drug use and alcohol abuse. The patient uses barrier protection occasionally when engaging in intercourse. On physical exam you note a murmur heard along the left mid-sternal border. The pulmonary exam reveals minor bibasilar crackles. Examination of the digits is notable for linea melanonychia. The patient's upper limbs demonstrate many bruises and scars in the antecubital fossa. Her temperature is 103.5°F (39.5°C), blood pressure is 100/70 mmHg, pulse is 112/min, respirations are 18/min, and oxygen saturation is 93% on room air. The patient's BMI is 16 kg/m^2. The patient is started on vancomycin and gentamicin and sent for echocardiography. Based on the results of echocardiography the patient is scheduled for surgery the next day. Vegetations are removed from the tricuspid valve during the surgical procedure and vancomycin and gentamicin are continued over the next 5 days. On post-operative day five, the patient presents with bleeding from her gums, oozing from her surgical sites, and recurrent epitaxis. Lab value are obtained as seen below: Serum: Na+: 135 mEq/L Cl-: 90 mEq/L K+: 4.4 mEq/L HCO3-: 23 mEq/L BUN: 20 mg/dL Glucose: 110 mg/dL Creatinine: 1.0 mg/dL Ca2+: 10.1 mg/dL AST: 9 U/L ALT: 9 U/L Leukocyte count and differential: Leukocyte count: 6,000 cells/mm^3 Lymphocytes: 20% Monocytes: 1% Neutrophils: 78% Eosinophils: 1% Basophils: 0% PT: 27 seconds aPTT: 84 seconds D-dimer: < 50 µg/L Hemoglobin: 14 g/dL Hematocrit: 40% Platelet count: 150,000/mm^3 Mean corpuscular volume: 110 fL Mean corpuscular hemoglobin concentration: 34 g/dL RDW: 14% Which of the following is the most likely cause of this patient's current symptoms?
An endocervical swab is performed and nucleic acid amplification testing via polymerase chain reaction is conducted. It is positive for Chlamydia trachomatis and negative for Neisseria gonorrhoeae. Which of the following is the most appropriate pharmacotherapy?
A 22-year-old man presents to clinic with a chief concern about a painless ulcer on his penis that he noticed 4 weeks ago and resolved one week ago. He denies any pain on urination or changes in urinary patterns. He admits to having multiple sexual partners in the past 3 months and inconsistent use of barrier protection. His vitals are within normal limits and his physical exam is unremarkable. He is given the appropriate antibiotic for this condition and sent home. What molecular structure is mimicked by the antibiotic most likely prescribed in this case?
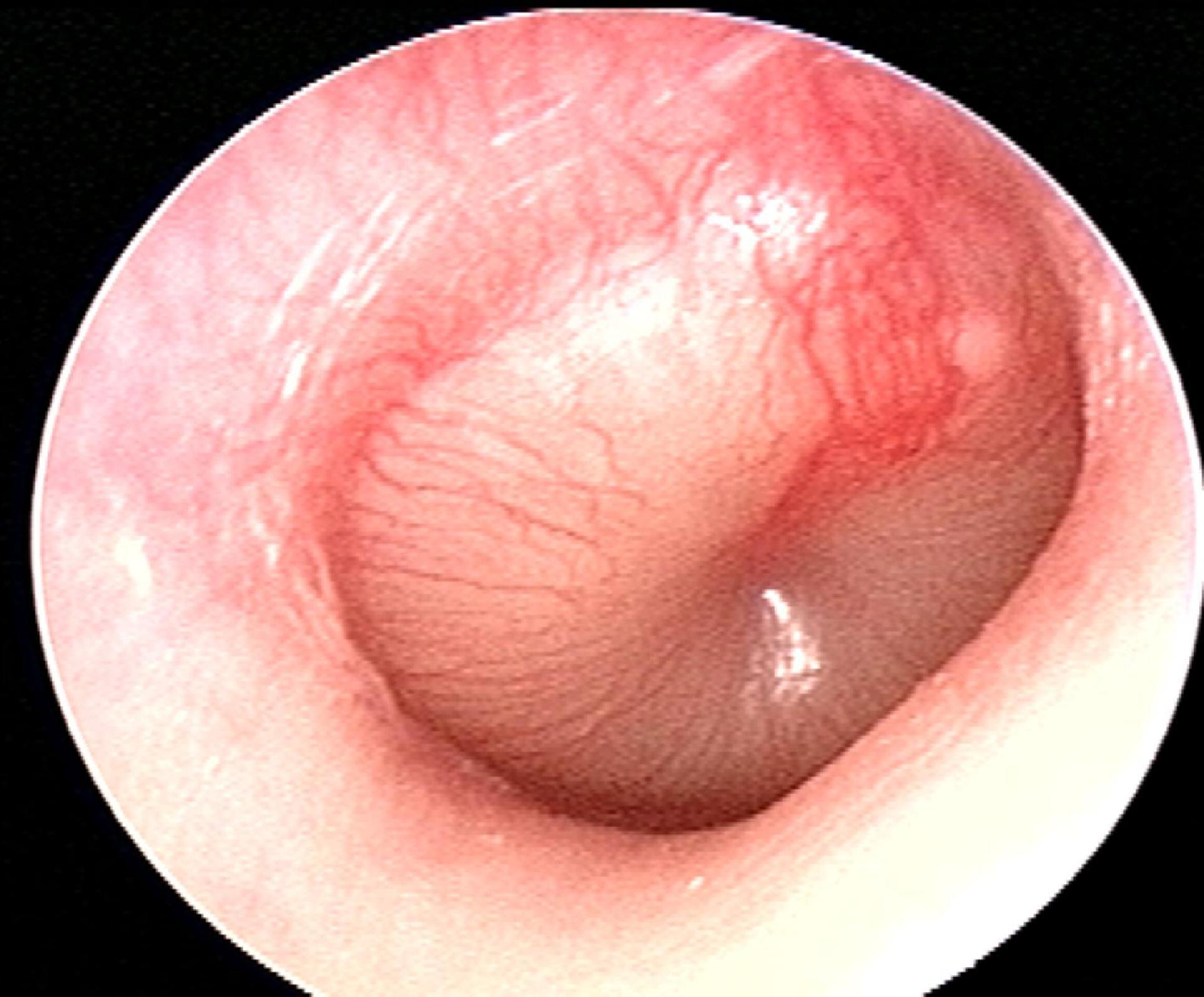
A 7-year-old boy is brought to the clinic by his parents due to right ear pain. For the past few days, the patient's parents say he has had a low-grade fever, a runny nose, and has been frequently pulling on his right ear. Past medical history is significant for a similar episode one month ago for which he has prescribed a 10-day course of amoxicillin. He is up-to-date on all vaccinations and is doing well at school. His temperature is 38.5°C (101.3°F), blood pressure is 106/75 mm Hg, pulse is 101/min, and respiratory rate is 20/min. Findings on otoscopic examination are shown in the image. The patient is treated with amoxicillin with clavulanic acid. Which of the following best describes the benefit of adding clavulanic acid to amoxicillin?
A 44-year-old woman presents to her primary care physician for worsening dysuria, hematuria, and lower abdominal pain. Her symptoms began approximately 2 days ago and have progressively worsened. She denies headache, nausea, vomiting, or diarrhea. She endorses feeling "feverish" and notes to having foul smelling urine. She has a past medical history of Romano-Ward syndrome and is not on any treatment. She experiences profuse diarrhea and nausea when taking carbapenems and develops a severe rash with cephalosporins. Her temperature is 100.4°F (38C), blood pressure is 138/93 mmHg, pulse is 100/min, and respirations are 18/min. On physical exam, the patient appears uncomfortable and there is tenderness to palpation around the bilateral flanks and costovertebral angle. A urinalysis and urine culture is obtained and appropriate antibiotics are administered. On her next clinical visit urine studies and a basic metabolic panel is obtained, which is shown below: Serum: Na+: 140 mEq/L Cl-: 101 mEq/L K+: 4.2 mEq/L HCO3-: 22 mEq/L BUN: 20 mg/dL Glucose: 94 mg/dL Creatinine: 2.4 mg/dL Urinalysis Color: Yellow Appearance: Clear Blood: Negative pH: 7 (Normal 5-8) Protein: Negative Nitrite: Negative Leukocyte esterase: Negative Cast: Epithelial casts FeNa: 3% Urine culture Preliminary report: 10,000 CFU/mL E. coli Which of the following antibiotics was most likely given to this patient?
Practice by Chapter
Penicillins and beta-lactamase inhibitors
Practice Questions
Cephalosporins
Practice Questions
Carbapenems and monobactams
Practice Questions
Fluoroquinolones
Practice Questions
Aminoglycosides
Practice Questions
Macrolides, ketolides, and lincosamides
Practice Questions
Tetracyclines and glycylcyclines
Practice Questions
Sulfonamides and trimethoprim
Practice Questions
Vancomycin and other glycopeptides
Practice Questions
Oxazolidinones and streptogramins
Practice Questions
Daptomycin and lipopeptides
Practice Questions
Polymyxins
Practice Questions
Antibiotic resistance mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app