
Antibiotics — MCQs

On this page
A patient weighing 70 kg (154 lb) requires intravenous antibiotics for a calcified abscess. The desired target plasma concentration of the antibiotic is 4.5 mg/L. The patient is estimated to have a volume of distribution of 30 L and a clearance rate of 60 mL/min. How many milligrams of the drug should be administered for the initial dose to reach the desired target plasma concentration?
An 8-year-old girl is brought to the emergency room for a 6-hour history of fever, sore throat, and difficulty swallowing. Physical examination shows pooling of oral secretions and inspiratory stridor. Lateral x-ray of the neck shows thickening of the epiglottis and aryepiglottic folds. Throat culture with chocolate agar shows small, gram-negative coccobacilli. The patient's brother is started on the recommended antibiotic for chemoprophylaxis. Which of the following is the primary mechanism of action of this drug?
A 13-year-old boy re-presents to his pediatrician with a new onset rash that began a few days after his initial visit. He initially presented with complaints of sore throat but was found to have a negative strep test. His mother demanded that he be placed on antibiotics, but this was refused by his pediatrician. The boy's father, a neurologist, therefore, started him on penicillin. Shortly after starting the drug, the boy developed a fever and a rash. The patient is admitted and his symptoms worsen. His skin begins to slough off, and the rash covers over 30% of his body. His oropharynx and corneal membranes are also affected. You examine him at the bedside and note a positive Nikolsky's sign. What is the most likely diagnosis?
A 45-year-old man presents to the physician with complaints of fever with rigors, headache, malaise, muscle pains, nausea, vomiting, and decreased appetite for the past 3 days. He informs the physician that he had been backpacking on the Appalachian Trail in the woods of Georgia in the month of June, 2 weeks ago, and had been bitten by a tick there. His temperature is 39.0°C (102.3°F), pulse is 94/min, respirations are 18/min, and blood pressure is 126/82 mm Hg. His physical exam does not reveal any significant abnormality except for mild splenomegaly. Laboratory studies show: Total white blood cell count 3,700/mm3 (3.7 x 109/L) Differential count Neutrophils 85% Lymphocytes 12% Monocytes 2% Eosinophils 1% Basophils 0% Platelet count 88,000/mm3 (95 x 109/L) Serum alanine aminotransferase 140 IU/L Serum aspartate aminotransferase 80 IU/L Microscopic examination of a peripheral blood smear stained with Wright-Giemsa stain shows the presence of morulae in the cytoplasm of leukocytes. In addition to drugs for symptomatic relief, what is the most appropriate initial step in the treatment of this patient?
A 22-year-old male presents to the physician with a 9-year history of recurring acne on his face. He has tried a number of over-the-counter face wash, gels, and supplements over the past few years with temporary relief but no significant lasting effects. The acne has gotten worse over time and now he is especially concerned about his appearance. A physical examination reveals numerous nodulocystic lesions over the face and neck. Scarring is present interspersed between the pustules. There are some lesions on the shoulders and upper back as well. Which of the following is the most appropriate treatment option for this patient at this time?
A 26-year-old woman comes to the emergency department with fever, abdominal pain, and nausea for the past 7 hours. The pain started in the right lower abdomen but has now progressed to diffuse abdominal pain. Her temperature is 39.5°C (103.1°F). Physical examination shows generalized abdominal tenderness with rebound, guarding, and decreased bowel sounds. She is taken for an emergency exploratory laparoscopy, which shows a perforated appendix with an adjacent abscess and peritoneal inflammation. Cultures from the abscess fluid grow catalase-producing, anaerobic, gram-negative rods that have the ability to grow in bile. Which of the following is the most appropriate pharmacotherapy for this patient?
An 8-year-old girl is brought to the emergency department because of a 2-day history of low-grade fever, itchy rash, and generalized joint pain. The rash initially started in the antecubital and popliteal fossae and then spread to her trunk and distal extremities. One week ago, she was diagnosed with acute sinusitis and was started on amoxicillin. She has no history of adverse drug reactions and immunizations are up-to-date. Her temperature is 37.5°C (99.5°F), pulse is 90/min, and blood pressure is 110/70 mm Hg. Physical examination shows periorbital edema and multiple erythematous, annular plaques of variable sizes over her entire body. One of the lesions in the right popliteal fossa has an area of central clearing and the patient's mother reports that it has been present for over 24 hours. Urinalysis is normal. Which of the following is the most likely diagnosis?
A 57-year-old HIV-positive male with a history of intravenous drug abuse presents to the emergency room complaining of arm swelling. He reports that he developed progressively worsening swelling and tenderness over the right antecubital fossa three days prior. He recently returned from a trip to Nicaragua. His past medical history is notable for an anaphylactoid reaction to vancomycin. His temperature is 101.4°F (38.6°C), blood pressure is 140/70 mmHg, pulse is 110/min, and respirations are 20/min. Physical examination reveals an erythematous, fluctuant, and tender mass overlying the right antecubital fossa. Multiple injection marks are noted across both upper extremities. He undergoes incision and drainage and is started on an antibiotic that targets the 50S ribosome. He is discharged with plans to follow up in one week. However, five days later he presents to the same emergency room complaining of abdominal cramps and watery diarrhea. Which of the following classes of pathogens is most likely responsible for this patient’s current symptoms?
A 70-year-old man presents to his primary care physician for ear pain. The patient states he has had ear pain for the past several days that seems to be worsening. The patient lives in a retirement home and previously worked as a banker. The patient currently is active, swims every day, and drinks 3 to 4 glasses of whiskey at night. There have been multiple cases of the common cold at his retirement community. The patient has a past medical history of myocardial infarction, Alzheimer dementia, diabetes, hypertension, vascular claudication, and anxiety. His current medications include insulin, metformin, aspirin, metoprolol, lisinopril, and buspirone. His temperature is 99.5°F (37.5°C), blood pressure is 167/108 mmHg, pulse is 102/min, respirations are 17/min, and oxygen saturation is 98% on room air. Cardiopulmonary exam is within normal limits. HEENT exam is notable for tenderness over the left mastoid process. Abdominal and musculoskeletal exam are within normal limits. Which of the following is the best management for this patient's condition?
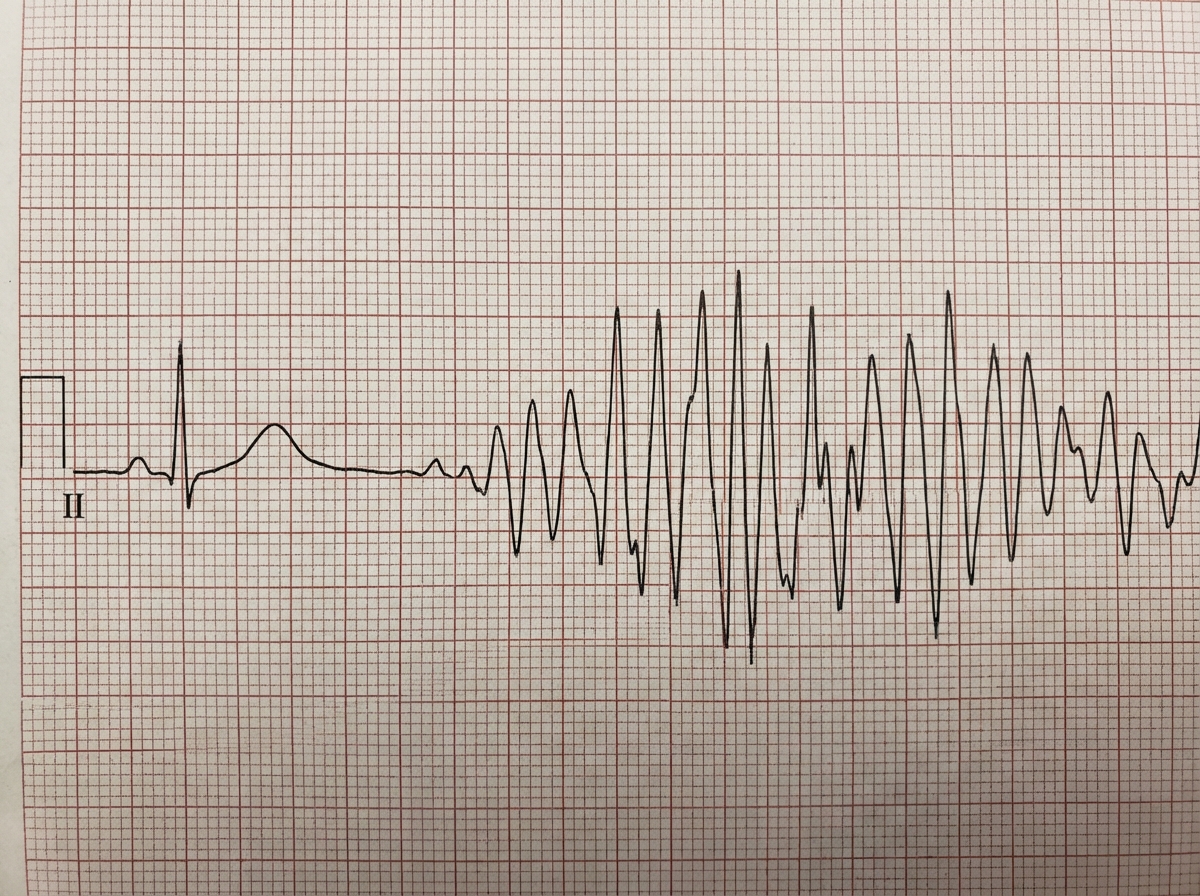
Four days into hospitalization for severe pneumonia, a 76-year-old woman suddenly becomes unresponsive. She has no history of heart disease. She is on clarithromycin and ceftriaxone. Her carotid pulse is not detected. A single-lead ECG strip is shown. Previous ECG shows QT prolongation. Laboratory studies show: Serum Na+ 145 mEq/L K+ 6.1 mEq/L Ca2+ 10.5 mg/dL Mg2+ 1.8 mEq/L Thyroid-stimulating hormone 0.1 μU/mL Cardiopulmonary resuscitation has been initiated. Which of the following is the most likely underlying cause of this patient's recent condition?
Practice by Chapter
Penicillins and beta-lactamase inhibitors
Practice Questions
Cephalosporins
Practice Questions
Carbapenems and monobactams
Practice Questions
Fluoroquinolones
Practice Questions
Aminoglycosides
Practice Questions
Macrolides, ketolides, and lincosamides
Practice Questions
Tetracyclines and glycylcyclines
Practice Questions
Sulfonamides and trimethoprim
Practice Questions
Vancomycin and other glycopeptides
Practice Questions
Oxazolidinones and streptogramins
Practice Questions
Daptomycin and lipopeptides
Practice Questions
Polymyxins
Practice Questions
Antibiotic resistance mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app