
Antibiotics — MCQs

On this page
Blood cultures are sent to the laboratory. Antibiotic treatment is started. Blood cultures confirm an infection with methicillin-susceptible Staphylococcus epidermidis in a patient with a prosthetic heart valve. Which of the following is the most appropriate next step in management?
A 45-year-old man presents to his primary care physician for lower extremity pain and unsteadiness. He describes the pain as severe and stabbing and affecting his lower extremities. These episodes of pain last for minutes at a time. He also reports knocking into furniture regularly. Medical history is significant for streptococcal pharyngitis, where he had a severe allergic reaction to appropriate treatment. He is currently sexually active with men and does not use condoms. On physical exam, his pupils are miotic in normal and low light. The pupils do not constrict further when exposed to the penlight and there is no direct or consensual pupillary dilation when the penlight is removed. The pupils constrict further when exposed to a near object. He has decreased vibration and proprioception sense in his lower extremities, absent lower extremity deep tendon reflexes, and a positive Romberg test. Which of the following is the best next step in management?
A 13-year-old girl presents with a right infected ingrown toenail. On examination, the skin on the lateral side of the toe is red, warm, swollen, and severely tender to touch. When gentle pressure is applied, pus oozes out. Culture and sensitivity analysis of the pus shows methicillin-resistant Staphylococcus aureus (MRSA). Which of the following antibiotics is most effective against this organism?
An 18-year-old man seeks an evaluation from a physician for painful right axillary swelling since 2 days ago. He has malaise. He has no history of serious illnesses and takes no medications. He has a pet kitten which was recently treated for fleas. The temperature is 38.5℃ (101.3℉), the pulse is 88/min, the respiration rate is 14/min, and the blood pressure is 120/80 mm Hg. There are 2 painless papules on the patient’s right forearm that appeared on the healing scratch marks left by his pet kitten a few days ago. Several lymph nodes in the right axilla are enlarged and tender. The overlying skin is erythematous. No other lymphadenopathy is detected in other areas. The rest of the examination shows no abnormalities. Which of the following is the most appropriate pharmacotherapy at this time?
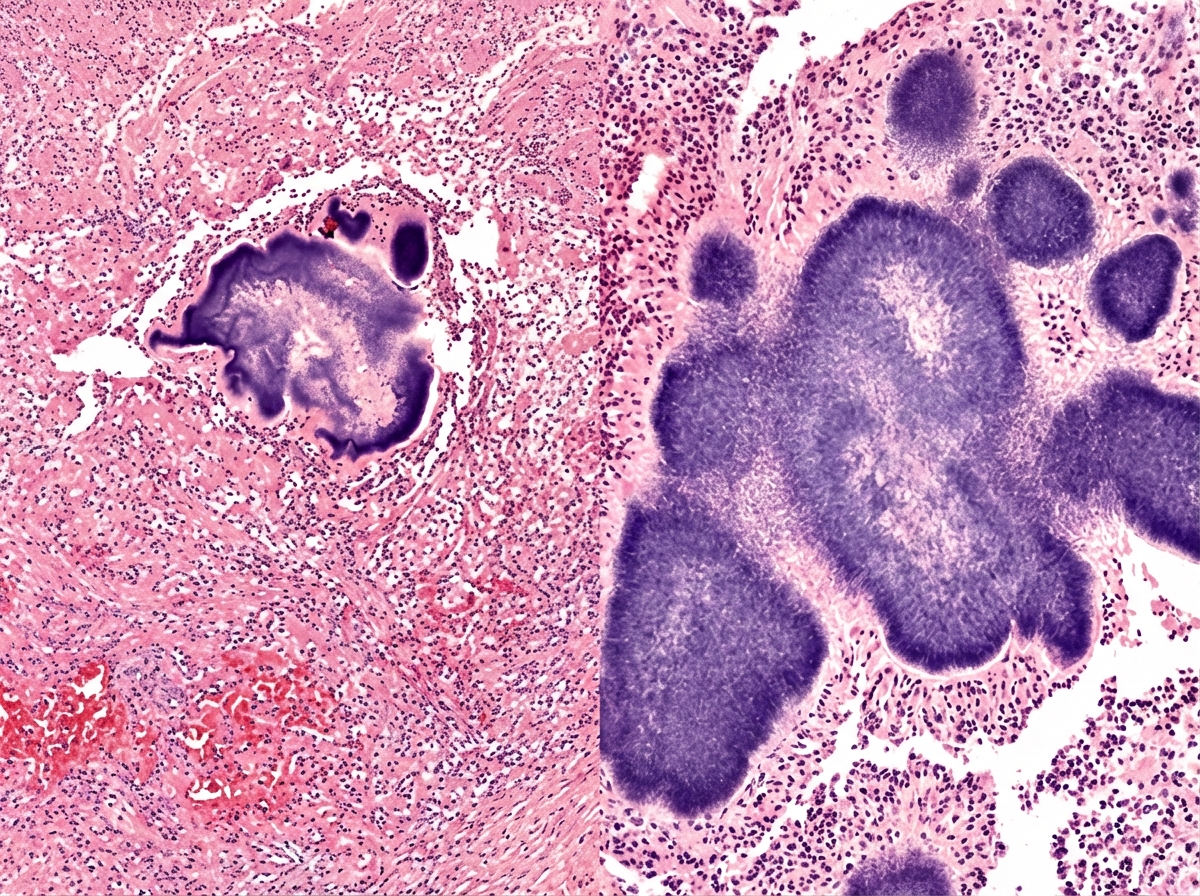
A 68-year-old man comes to the physician because of a 3-month history of anorexia, weight loss, and cough productive of blood-tinged sputum with yellow granules. Four months ago he was treated for gingivitis. He has smoked 1 pack of cigarettes daily for 40 years. Examination shows crackles over the right upper lung field. An x-ray of the chest shows a solitary nodule and one cavitary lesion in the right upper lung field. A photomicrograph of a biopsy specimen from the nodule obtained via CT-guided biopsy is shown. Which of the following is the most appropriate pharmacotherapy?
A 30-year-old man is diagnosed with multi-drug resistant tuberculosis after a recent trip to Eastern Europe. After drug susceptibility testing is completed, he is given a regimen of antibiotics as treatment. He returns two weeks later complaining of decreased visual acuity and color-blindness. What is the mechanism of action of the drug that is most likely to cause this side effect?
A 67-year-old African American male presents to the emergency room complaining of nausea and right flank pain. He reports that these symptoms have worsened over the past two days. His past medical history is notable for congestive heart failure, hypertension, hyperlipidemia, and diabetes mellitus. He currently takes aspirin, losartan, metoprolol, atorvastatin, hydrochlorothiazide, furosemide, and metformin. He is allergic to fluoroquinolones. His temperature is 102.9°F (39.4°C), blood pressure is 100/50 mmHg, pulse is 120/min, and respirations are 28/min. On exam, he demonstrates right costovertebral angle tenderness. Urinalysis reveals 30 WBCs/hpf and positive leukocyte esterase. He is admitted and started on a broad-spectrum combination intravenous antibiotic. He recovers well and is discharged with plans to follow up in 2 weeks. At his follow-up, he reports that he has developed transient visual blurring whenever he turns his head to the right or left. He also reports that he has fallen at home multiple times. What is the mechanism of action of the drug that is most likely responsible for this patient’s current symptoms?
A 62-year-old man presents with epigastric pain over the last 6 months. He says the pain gets worse with food, especially coffee. He also complains of excessive belching. He says he has tried omeprazole recently, but it has not helped. No significant past medical history or current medications. On physical examination, there is epigastric tenderness present on deep palpation. An upper endoscopy is performed which reveals gastric mucosa with signs of mild inflammation and a small hemorrhagic ulcer in the antrum. A gastric biopsy shows active inflammation, and the specimen stains positive with Warthin–Starry stain, revealing Helicobacter pylori. Which of the following is the next, best step in the management of this patient’s condition?
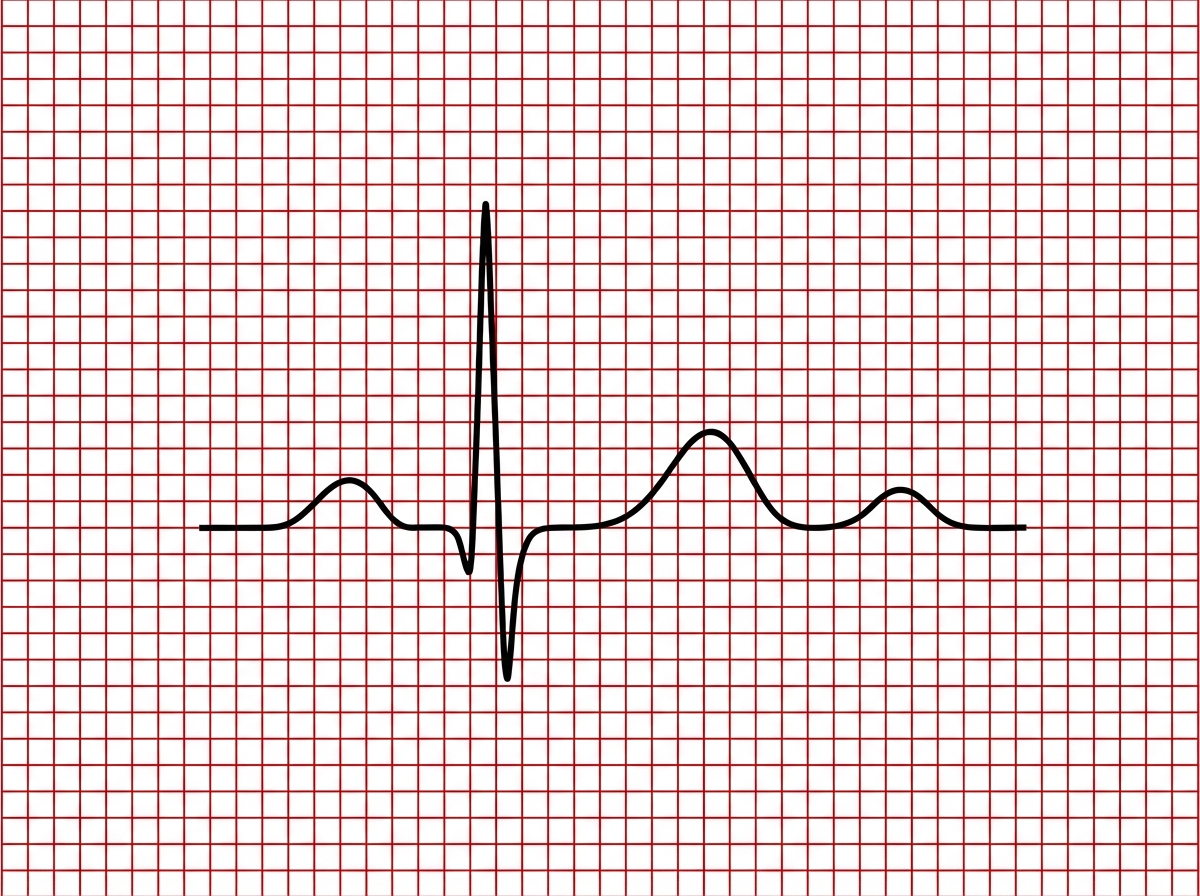
A 48-year-old woman is admitted to the hospital with sepsis and treated with gentamicin. One week after her admission, she develops oliguria and her urine shows muddy brown casts on light microscopy. Days later, her renal function begins to recover, but she complains of weakness and develops U waves on EKG as shown in Image A. Which laboratory abnormality would you most expect to see in this patient?
A 34-year-old man comes to the physician for a 1-week history of fever and generalized fatigue. Yesterday, he developed a rash all over his body. Two months ago, he had a painless lesion on his penis that resolved a few weeks later without treatment. He has asthma. Current medications include an albuterol inhaler. He is currently sexually active with 3 different partners. He uses condoms inconsistently. Vital signs are within normal limits. He has a diffuse maculopapular rash involving the trunk, extremities, palms, and soles. An HIV test is negative. Rapid plasma reagin (RPR) and fluorescent treponemal antibody absorption test (FTA-ABS) are positive. The patient receives a dose of intramuscular benzathine penicillin G. Two hours later, he complains of headache, myalgias, and chills. His temperature is 38.8°C (101.8°F) , pulse is 105/min, respirations are 24/min, and blood pressure is 98/67 mm Hg. Which of the following is the most appropriate pharmacotherapy?
Practice by Chapter
Penicillins and beta-lactamase inhibitors
Practice Questions
Cephalosporins
Practice Questions
Carbapenems and monobactams
Practice Questions
Fluoroquinolones
Practice Questions
Aminoglycosides
Practice Questions
Macrolides, ketolides, and lincosamides
Practice Questions
Tetracyclines and glycylcyclines
Practice Questions
Sulfonamides and trimethoprim
Practice Questions
Vancomycin and other glycopeptides
Practice Questions
Oxazolidinones and streptogramins
Practice Questions
Daptomycin and lipopeptides
Practice Questions
Polymyxins
Practice Questions
Antibiotic resistance mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app