
Antibiotics — MCQs

On this page
A 22-year-old woman presents to the doctor's office seeking evaluation for her recurrent urinary tract infections. She admits to urinary frequency and a burning sensation when urinating. This is her 3rd UTI in the past year. She has a history of generalized anxiety disorder for which she takes paroxetine. She is sexually active and has had multiple partners during the past year. The patient’s blood pressure is 116/72 mm Hg, the heart rate is 76/min, the respiratory rate is 12/min and the temperature is 36.8°C (98.2°F). On physical examination, she is alert and oriented to time, place, and person. There is no murmur. Her lungs are clear to auscultation bilaterally. Her abdomen is soft and non-tender to palpation. The distance from the urethra to anus is shorter than the average female her age. Urinalysis and urine culture results are provided: Urine culture results 200 CFUs of Escherichia coli (normal < 100 if symptomatic) Leukocyte esterase positive WBC 50-100 cells/hpf Nitrite positive RBC 3 cells/hpf Epithelial cells 2 cells/hpf pH 5.2 (normal 4.5–8) Which of the following recommendations would be most appropriate for this patient?
A 41-year-old homeless man is brought to the emergency department complaining of severe fever, dizziness, and a persistent cough. The patient has a history of long-standing alcohol abuse and has frequently presented to the emergency department with acute alcohol intoxication. The patient states that his cough produces ‘dark brown stuff’ and he provided a sample for evaluation upon request. The patient denies having any other underlying medical conditions and states that he has no other symptoms. He denies taking any medications, although he states that he knows he has a sulfa allergy. On observation, the patient looks frail and severely fatigued. The vital signs include: blood pressure 102/72 mm Hg, pulse 98/min, respiratory rate 15/min, and temperature 37.1°C (98.8°F). Auscultation reveals crackles in the left upper lobe and chest X-ray reveals an infiltrate in the same area. Which of the following is the most appropriate treatment for this patient?
A 51-year-old man is admitted to the hospital because of a 2-day history of fever, nausea, and abdominal pain. His temperature is 39.4°C (102.9°F) and pulse is 106/min. Physical examination shows tenderness in the right upper quadrant. Blood cultures grow nonhemolytic, gram-positive cocci that grow in hypertonic saline. Antibiotic sensitivity testing of the isolated organism shows that gentamicin has a minimum inhibitory concentration (MIC) of 16 μg/mL. The addition of ampicillin, which has an MIC of 2 μg/mL alone, decreases the MIC of gentamicin to 0.85 μg/mL. The decrease in the MIC of gentamicin with the addition of ampicillin is most likely due to which of the following mechanisms?
A 42-year-old woman with a history of multiple sclerosis and recurrent urinary tract infections comes to the emergency department because of flank pain and fever. Her temperature is 38.8°C (101.8°F). Examination shows left-sided costovertebral angle tenderness. She is admitted to the hospital and started on intravenous vancomycin. Three days later, her symptoms have not improved. Urine culture shows growth of Enterococcus faecalis. Which of the following best describes the most likely mechanism of antibiotic resistance in this patient?
A 56-year-old man presents with breathlessness and altered mental status. The patient’s daughter says that he has been having high fever and cough for the last 3 days. Past medical history is significant for a recent hospitalization 5 days ago, following a successful coronary artery bypass grafting (CABG). In the post-operative period, he was in an intensive care unit (ICU) for 6 days, including 12 hours on mechanical ventilation. Current medications are aspirin and rosuvastatin. The patient’s daughter mentions that he has had anaphylactic reactions to penicillin in the past. His temperature is 39.4°C (103°F), pulse rate is 110/min, blood pressure is 104/78 mm Hg, and respiratory rate is 30/min. On physical examination, the patient is confused and disoriented and shows signs of respiratory distress and cyanosis. On chest auscultation, there is crepitus in the right lung. The patient is immediately started on oxygen therapy, intravenous fluids, and supportive care. After the collection of appropriate samples for bacteriological culture, treatment with empirical intravenous antibiotics are started. After 24 hours of treatment, the microbiology results indicate Pseudomonas aeruginosa infection. Antibiotic therapy is changed to a combination of aztreonam and tobramycin. Which of the following best describes the rationale for choosing this antibiotic combination?
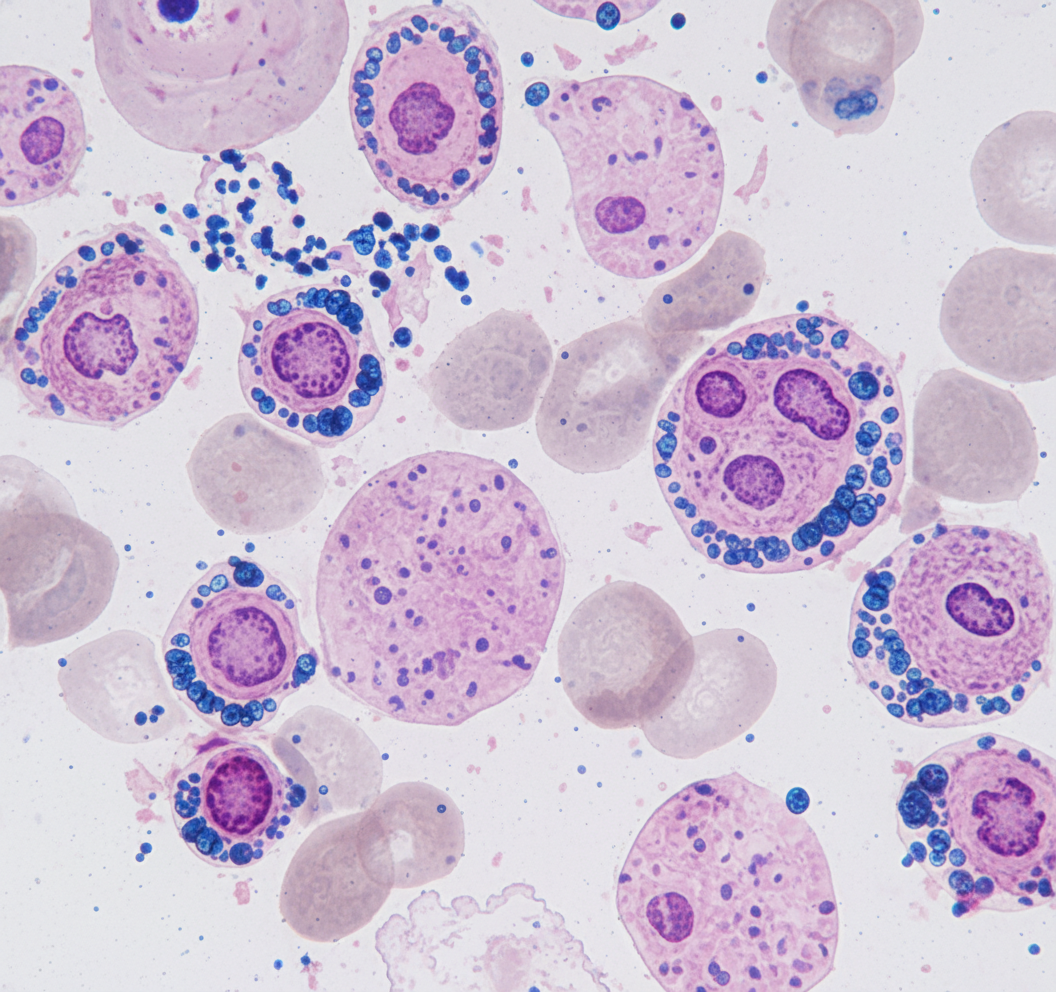
A 46-year-old man who recently immigrated from Mexico comes to the physician for a pre-employment wellness examination. A tuberculin skin test is administered and he develops 12 mm of palpable induration, with or without surrounding erythema, on his forearm within 48 hours. An x-ray of the chest shows no abnormalities. He is started on the recommended antibiotic treatment for latent tuberculosis. Four weeks later, he returns for a follow-up examination. Laboratory studies show a hemoglobin concentration of 9.3 g/dL, serum alanine aminotransferase activity of 86 U/L, and serum aspartate aminotransferase activity of 66 U/L. A photomicrograph of a Prussian blue-stained bone marrow smear is shown. Which of the following is the mechanism of action of the drug responsible for this patient's findings?
A 49-year-old man presents to the emergency department with acute onset of pain and redness of the skin of his lower leg for the past 3 days. He has had type 2 diabetes mellitus for the past 12 years, but he is not compliant with his medications. He has smoked 10–15 cigarettes per day for the past 20 years. His temperature is 38°C (100.4°F), pulse is 95/min, and blood pressure is 110/70 mm Hg. On physical examination, the pretibial area is erythematous, edematous, and tender. He is diagnosed with acute cellulitis, and intravenous ceftazidime sodium is started. On the 5th day of antibiotic therapy, the patient complains of severe watery diarrhea, fever, and abdominal tenderness without rigidity. Complete blood count is ordered for the patient and shows 14,000 white blood cells/mm3. Which of the following is the best initial therapy for this patient?
A 28-year-old gravida 2 para 1 is receiving care from her obstetrician at 28 weeks. She states that she has been having suprapubic pain and urinary frequency for the past week. Her past medical history is significant for dermatomyositis for which she takes prednisone every day. She does not smoke cigarettes or drinks alcohol. Her vital signs are within normal limits. Physical examination of the patient is within normal limits. A urine sample from the patient shows > 100,000 CFU of Escherichia coli. Urinalysis results are provided as follows: Leukocyte esterase positive WBC 50-100 cells/HPF Nitrite positive RBC 2 cells/HPF Epithelial cells 2 cells/HPF Urine pH 5.2 Which of the following is the best pharmacotherapy for this patient’s condition?
A 26-year-old woman presents to her primary care physician because she has been experiencing occasional fevers and chills for the last 3 weeks. She says that the fevers have been accompanied by abdominal pain and increased vaginal discharge. On presentation her temperature is 101.0°F (38.3°C), blood pressure is 113/75 mmHg, pulse is 105/min, and respirations are 12/min. On physical exam she is found to have tenderness over the lower abdominal quadrants, and speculum exam shows uterine inflammation as well as a retained intrauterine device. The most likely cause of this patient's symptoms should be treated with an antibiotic with which mechanism of action?
A 24-year-old woman comes to the physician because of a 3-day history of lower abdominal pain and dysuria. She has a history of recurring urinary tract infections that have resolved with antibiotic treatment. She is sexually active with one male partner and they do not use condoms. She had mild pain during her last sexual intercourse one week ago. Her temperature is 38.2°C (100.8°F), pulse is 86/min, and blood pressure is 110/70 mm Hg. Physical examination shows lower abdominal tenderness and bilateral inguinal lymphadenopathy. There is a small amount of purulent vaginal discharge. Bimanual examination shows uterine and cervical motion tenderness. Laboratory studies show: Hemoglobin 12 g/dL Leukocyte count 13,500/mm3 Segmented neutrophils 75% Eosinophils 1% Lymphocytes 22% Monocytes 2% Platelet count 328,000/mm3 Erythrocyte sedimentation rate 82 mm/h Urine RBC 1–2/hpf WBC 0–1/hpf Nitrite negative Bacteria occasional Urine pregnancy test negative Which of the following is the most appropriate pharmacotherapy?
Practice by Chapter
Penicillins and beta-lactamase inhibitors
Practice Questions
Cephalosporins
Practice Questions
Carbapenems and monobactams
Practice Questions
Fluoroquinolones
Practice Questions
Aminoglycosides
Practice Questions
Macrolides, ketolides, and lincosamides
Practice Questions
Tetracyclines and glycylcyclines
Practice Questions
Sulfonamides and trimethoprim
Practice Questions
Vancomycin and other glycopeptides
Practice Questions
Oxazolidinones and streptogramins
Practice Questions
Daptomycin and lipopeptides
Practice Questions
Polymyxins
Practice Questions
Antibiotic resistance mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app