
Growth/Development — MCQs

On this page
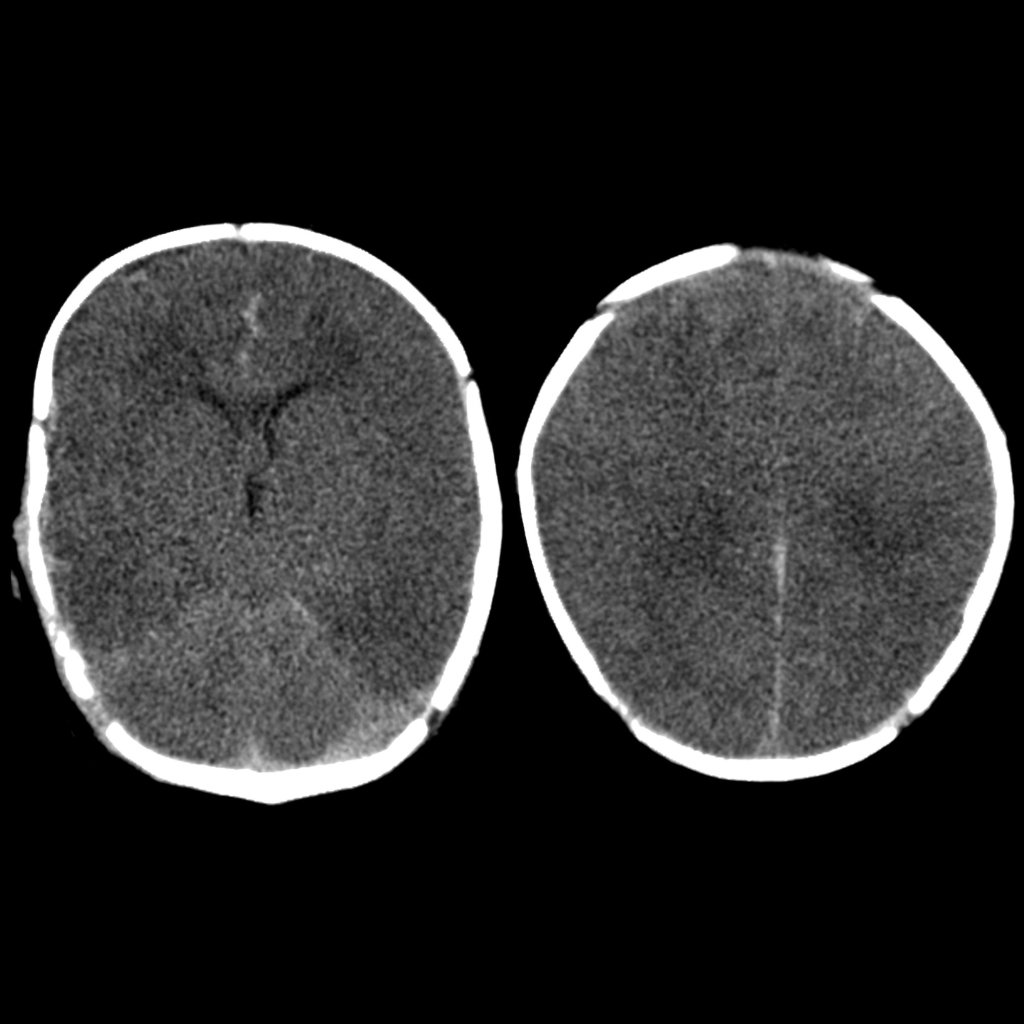
A 10-month-old infant is brought to the emergency by his parents after a seizure. The parents report no history of trauma, fever, or a family history of seizures. However, they both say that the patient fell while he was running. Neurologic examination was normal. A head CT scan was ordered and is shown in figure A. Which of the following is most likely found in this patient?
A 10-year-old girl is brought to the emergency department because of lower abdominal pain for the past 12 hours. The pain has progressively worsened and was accompanied by occasional episodes of diarrhea. She has vomited twice. Her mother has Crohn disease. Her temperature is 38.1°C (100.6°F), pulse is 95/min, respirations are 20/min, and blood pressure is 110/70 mm Hg. The abdomen is soft, and there is mild tenderness to palpation in the right lower quadrant without rebound or guarding. Bowel sounds are normal. Her hemoglobin concentration is 13.0 g/dL, leukocyte count is 12,800/mm3, and platelet count is 345,000/mm3. Urine dipstick is negative for nitrites and leukocyte esterase. Urinalysis shows 3 WBC/hpf and no RBCs. Which of the following is the most appropriate next step in management?
A 16-year-old boy is brought to the physician for a follow-up examination. He has a 6-year history of type 1 diabetes mellitus and his only medication is insulin. Seven months ago, he was treated for an episode of diabetic ketoacidosis. He has previously been compliant with his diet and insulin regimen. He wants to join the high school soccer team. Vital signs are within normal limits. His hemoglobin A1C is 6.3%. Which of the following is the most appropriate recommendation at this time?
A 5-week-old male infant is rushed to the emergency department due to severe vomiting and lethargy for the past 3 days. His mother describes the vomiting as forceful and projectile and contains undigested breast milk, but she did not notice any green fluids. He has not gained much weight in the past 3 weeks and looks very thin. He has a pulse of 144/min, temperature of 37.5°C (99.5°F), and respiratory rate of 18/min. Mucous membranes are dry and the boy is lethargic. Abdominal examination reveals a palpable mass in the epigastrium that becomes more prominent after vomiting with visible peristaltic movements over the epigastrium. Barium-contrast studies show a double channel appearance of the pylorus. What is the best immediate step in the management of this patient’s condition?
A concerned father brings his 2 year-old son to the clinic for evaluation. In the past 24 hours, the child has had multiple episodes of painless bloody stools. On physical examination, the child's vital signs are within normal limits. There is mild generalized discomfort on palpation of the abdomen but no rebound or guarding. A technetium-99m (99mTc) pertechnetate scan indicates increased activity in two locations within the abdomen. Cells originating in which organ account for the increased radionucleotide activity?
A 3-month-old male presents to the pediatrician with his mother for a well child visit. The patient drinks 4 ounces of conventional cow’s milk formula every three hours. He usually stools once per day, and urinates up to six times per day. His mother reports that he regurgitates a moderate amount of formula through his nose and mouth after most feeds. He does not seem interested in additional feeding after these episodes of regurgitation, and he has become progressively more irritable around meal times. The patient is starting to refuse some feeds. His mother denies ever seeing blood or streaks of red in his stool, and she denies any family history of food allergies or dermatological problems. The patient’s weight was in the 75th percentile for weight throughout the first month of life. Four weeks ago, he was in the 62nd percentile, and he is now in the 48th percentile. His height and head circumference have followed similar trends. On physical exam, the patient smiles reciprocally and can lift his head and chest when in the prone position. His abdomen is soft, non-tender, and non-distended. Which of the following is the best next step in management?
An 8-month-old boy is brought to the emergency department by his mother and father due to decreasing activity and excessive sleepiness. The patient was born at full-term in the hospital with no complications. The patient's parents appear incredibly worried as their son has had no medical issues in the past. They show you videos of the child happily playing with his parents the day before. The patient's mother states that the patient hit his head while crawling this morning and since then has been difficult to arouse. His mother is worried because she thinks he had a fever earlier in the day and he was clutching his head and neck in pain. Physical examination shows a barely arousable boy with a large, full anterior fontanelle. The boy grimaces on palpation of his chest, and a radiograph shows posterior rib fractures. Retinal examination shows bilateral retinal hemorrhages. Which of the following is the most likely cause for this patient's presentation?
A 4-year-old girl is brought to the physician with a 3-month history of progressive intermittent pain and swelling involving both knees, right ankle, and right wrist. The patient has been undergoing treatment with acetaminophen and ice packs, both of which relieved her symptoms. The affected joints feel "stuck" and are difficult to move immediately upon waking up in the morning. However, the patient can move her joints freely after a few minutes. She also complains of occasional mild eye pain that resolves spontaneously. Five months ago, she was diagnosed with an upper respiratory tract infection that resolved without treatment. Vital signs are within normal limits. Physical examination shows swollen and erythematous joints, which are tender to touch. Slit-lamp examination shows an anterior chamber flare with signs of iris inflammation bilaterally. Laboratory studies show: Blood parameters Hemoglobin 12.6 g/dL Leukocyte count 8,000/mm3 Segmented neutrophils 76% Eosinophils 1% Lymphocytes 20% Monocytes 3% Platelet count 360,000/mm3 Erythrocyte sedimentation rate 36 mm/hr Serum parameters Antinuclear antibodies 1:320 Rheumatoid factor negative Which of the following is the most likely diagnosis?
A 4-week-old male infant is brought to the physician due to a 1-week history of refusing to finish bottle feeds and becoming irritable shortly after feeding. He spits up sour-smelling milk after most feeds. Pregnancy and delivery were uncomplicated. The baby is at the 70th percentile for length and 50th percentile for weight. His temperature is 36.6°C (98°F), pulse is 180/min, respirations are 30/min, and blood pressure is 85/55 mm Hg. He appears lethargic. Examination shows sunken fontanelles and a strong rooting reflex. The abdomen is soft with a 1.5-cm nontender epigastric mass. Which of the following is the most appropriate next step in the management of this patient?
A mother brings her 10 month-old boy to the pediatrician for a check-up. His birth was without complications and his development to-date has been progressing normally. He currently crawls, pulls himself up to standing, says 'mama' and 'dada' nonspecifically, and responds when called by his name. However, his mother is concerned, as she has noted over the past several weeks that he has periods where he stops breathing when he gets frightened or upset. These episodes last for 20-30 seconds and are accompanied by his lips and face becoming bluish. His breathing has always resumed normally within 45 seconds after the start of the episode, and he acts normally afterwards. One instance resulted in the child passing out for a 5-10 seconds before a spontaneous recovery. Which of the following is the most appropriate management of this patient's condition?
Practice by Chapter
Normal growth patterns
Practice Questions
Growth charts and interpretation
Practice Questions
Failure to thrive evaluation
Practice Questions
Short stature workup
Practice Questions
Tall stature evaluation
Practice Questions
Obesity in children
Practice Questions
Nutritional assessment tools
Practice Questions
Puberty stages (Tanner stages)
Practice Questions
Precocious puberty
Practice Questions
Delayed puberty
Practice Questions
Growth hormone disorders
Practice Questions
Impact of chronic disease on growth
Practice Questions
Catch-up growth
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app