
Growth/Development — MCQs

On this page
A 5-year-old boy is brought to the physician because of early morning headaches for the past 6 months. During this period, he has had severe nausea and occasional episodes of vomiting. For the past month, he has had difficulty walking and intermittent double vision. He was born at term and has been healthy apart from an episode of sinusitis 8 months ago that resolved spontaneously. He is at the 60th percentile for height and 50th percentile for weight. His temperature is 37.1°C (98.8°F), pulse is 80/min, and blood pressure is 105/64 mm Hg. Examination shows normal muscle strength and 2+ deep tendon reflexes bilaterally. He has a broad-based gait and impaired tandem gait. Fundoscopy shows bilateral swelling of the optic disc. There is esotropia of the left eye. Which of the following is the most likely diagnosis?
A 15-year-old boy is brought to the physician for a well-child visit. His parents are concerned that he has not had his growth spurt yet. As a child, he was consistently in the 60th percentile for height; now he is in the 25th percentile. His classmates make fun of his height and high-pitched voice. His parents are also concerned that he does not maintain good hygiene. He frequently forgets to shower and does not seem aware of his body odor. As an infant, he had bilateral orchidopexy for cryptorchidism and a cleft palate repair. He is otherwise healthy. Vital signs are within normal limits. On physical exam, axillary and pubic hair is sparse. Genitals are Tanner stage 1 and the testicles are 2 mL bilaterally. Which of the following is the most likely diagnosis?
A 6-month-old boy is brought to the emergency department by his mother, who informs the doctor that her alcoholic husband hit the boy hard on his back. The blow was followed by excessive crying for several minutes and the development of redness in the area. On physical examination, the boy is dehydrated, dirty, and irritable and when the vital signs are checked, they reveal tachycardia. He cries immediately upon the physician touching the area around his left scapula. The doctor strongly suspects a fracture of the 6th, 7th, or 8th retroscapular posterior ribs. Evaluation of his skeletal survey is normal. The clinician is concerned about child abuse in this case. Which of the following is the most preferred imaging technique as the next step in the diagnostic evaluation of the infant?
A 7-year-old boy is brought to the physician by his parents because of a 4.5-kg (10-lb) weight loss during the last 3 months. During this period, he has complained of abdominal pain and fullness, and his parents feel that he has been eating less. His parents also report that his urine has appeared pink for several weeks. He has been performing poorly in school lately, with reports from teachers that he has not been paying attention in class and has been distracting to other students. He was born at term and has been healthy except for a history of several infantile seizures. His vital signs are within normal limits. He is at the 60th percentile for height and 20th percentile for weight. Physical examination shows a palpable abdominal mass, abdominal tenderness in the left upper quadrant, and left costovertebral angle tenderness. There are several ellipsoid, hypopigmented macules on the back and legs and a 4-cm raised plaque of rough, dimpled skin on the right lower back that is the same color as the surrounding skin. Which of the following is the most likely diagnosis?
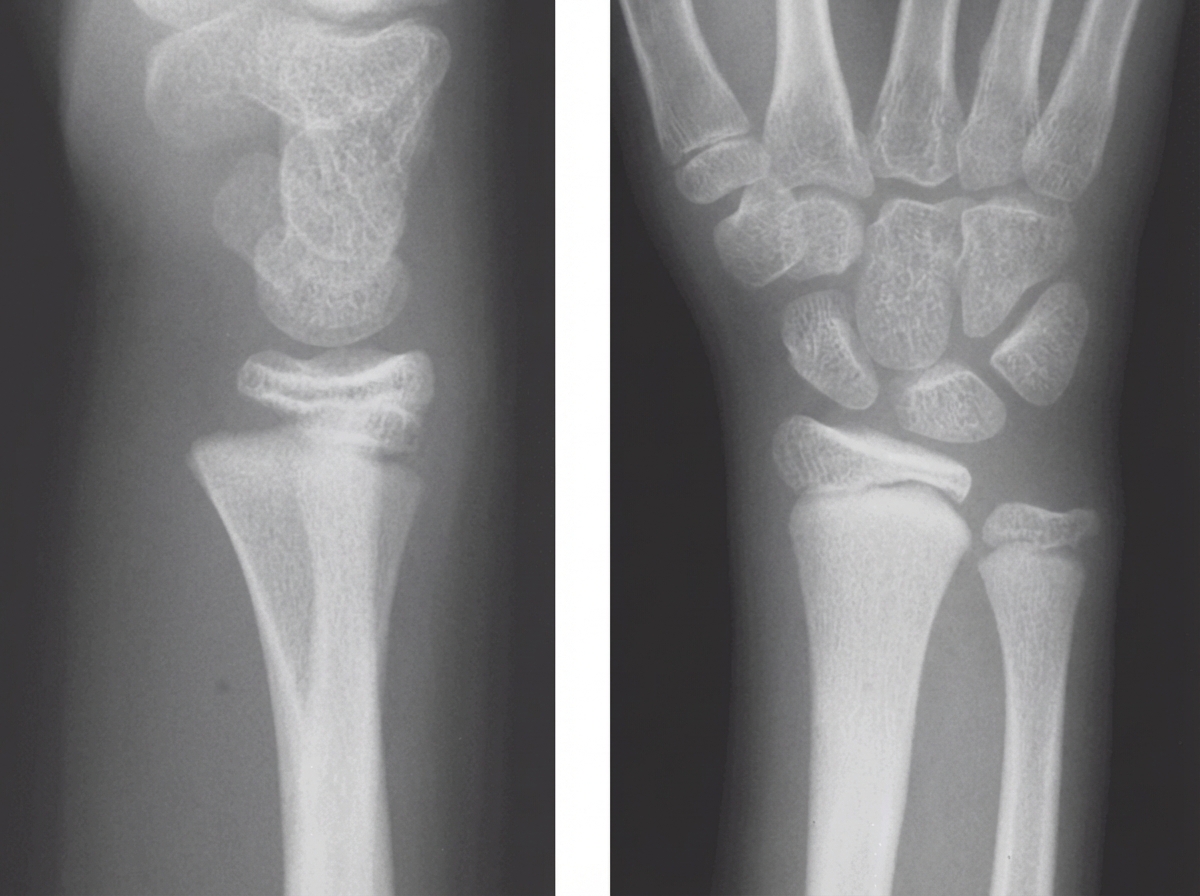
A 6-year-old refugee with delayed growth and weakness is brought to the physician. Her family has been displaced several times over the last few years, and nutrition and housing were frequently inadequate. Examination of the lower limbs shows bowing of the legs with reduced proximal muscle strength. The abdomen is protruded. Inspection of the chest shows subcostal grooving during inspiration. An image of the patient’s wrist is shown. Which of the following is the most likely cause of this patient’s condition?
A 5-year-old is brought into your office by his mother. His mother states that he is having 10-20 episodes per day where he stops responding to his mother and is found staring out of the window. During these periods, he blinks more frequently than normal, but returns to his normal self afterwards. These episodes last 30 to 60 seconds. His mother states that all of his milestones have been normal and he had an uncomplicated birth. His mother also denies any other recent illness. On exam, his vitals are normal. During one of these episodes in the office, his EEG shows three-per-second spike and wave discharge. What is the most likely diagnosis?
A 6-year-old girl is brought to the physician for a well-child examination. There is no personal or family history of serious illness. She is at the 90th percentile for height and weight. Vital signs are within normal limits. Examination shows enlarged breast buds that extend beyond the areola. There is coarse pubic hair that does not extend onto the inner thigh. The remainder of the examination show no abnormalities. An x-ray of the left hand shows a bone age of 10 years. Following GnRH agonist stimulation, serum luteinizing hormone levels increase to twice the median. Which of the following is the most appropriate next best step in management?
A 7-year-old girl is brought to the physician because of vaginal bleeding for 2 days. There is no personal or family history of serious illness. She is at the 95th percentile for height and at the 90th percentile for weight. Examination shows enlarged breasts, and the areola and papilla have formed a secondary mound. There is coarse pubic hair that does not extend to the inner thigh. The remainder of the examination show no abnormalities. An x-ray of the left hand and wrist shows a bone age of 11 years. Her serum luteinizing hormone concentration is 0.1 mIU/mL (N < 0.2 mIU/mL). Which of the following is the most appropriate next step in management?
An 18-month-old toddler is brought to a pediatric hematologist by his father. The boy was referred to this office for prolonged neutropenia. He has had several blood tests with an isolated low neutrophil count while hemoglobin, hematocrit, and platelet count is normal. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Today his complete blood count (CBC) with differential shows: Hemoglobin: 15.5 g/dL Platelets: 300,000 mm3 Neutrophils: 20% Bands: 2% Lymphocytes: 40% Monocytes: 15% Today, he has a heart rate of 90/min, respiratory rate of 22/min, blood pressure of 110/65 mm Hg, and temperature of 37.0°C (98.6°F). On physical exam, the child appears healthy and is within expected growth parameters for his age and sex. A bone marrow biopsy shows normal bone marrow with 95% cellularity and trilineage maturation. Flow cytometry is normal with no abnormal markers noted. Which of the following is the most probable diagnosis in the present case?
A 1-month-old boy is brought to the physician because of a 5-day history of generalized fatigue and multiple episodes of vomiting which is most pronounced after formula feeding. His vomiting progressed from 2–3 episodes on the first day to 6–8 episodes at present. The vomitus is whitish in color. The mother reports that he has been very hungry after each episode of vomiting. The patient was born at 38 weeks' gestation and weighed 3100 g (6 lb 13 oz); he currently weighs 3500 g (7 lb 11 oz). He appears irritable. His temperature is 37.1°C (98.8°F), pulse is 130/min, respirations are 43/min, and blood pressure is 74/36 mm Hg. Examination shows dry mucous membranes. The abdomen is soft and not distended. There is a round mass palpable in the epigastric region. The liver is palpated 1 cm below the right costal margin. Laboratory studies show: Hemoglobin 15.3 g/dL Leukocyte count 6300/mm3 Platelet count 230,000/mm3 Serum Na+ 133 mEq/L K+ 3.4 mEq/L Cl- 92 mEq/L Glucose 77 mg/dL Creatinine 1.0 mg/dL A urinalysis shows a decreased pH. Which of the following is the most appropriate next step in the management of this patient?
Practice by Chapter
Normal growth patterns
Practice Questions
Growth charts and interpretation
Practice Questions
Failure to thrive evaluation
Practice Questions
Short stature workup
Practice Questions
Tall stature evaluation
Practice Questions
Obesity in children
Practice Questions
Nutritional assessment tools
Practice Questions
Puberty stages (Tanner stages)
Practice Questions
Precocious puberty
Practice Questions
Delayed puberty
Practice Questions
Growth hormone disorders
Practice Questions
Impact of chronic disease on growth
Practice Questions
Catch-up growth
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app