
Growth/Development — MCQs

On this page
A 10-year-old boy is brought in by his parents with increasing breathlessness. He was diagnosed with asthma about 2 years ago and has been on treatment since then. He was initially observed to have breathlessness, cough and chest tightness 2 or 3 times a week. He would wake up once or twice a month in the nighttime with breathlessness. At that time, his pediatrician started him on a Ventolin inhaler to be used during these episodes. His symptoms were well controlled until a few months ago when he started to experience increased nighttime awakenings due to breathlessness. He is unable to play outside with his friends as much because he gets winded easily and has to use his inhaler almost daily to help him breathe easier. He is able to walk and perform other routine activities without difficulty, but playing or participating in sports causes significant struggles. Based on his symptoms, his pediatrician adds an inhaled formoterol and budesonide combination to his current regime. During spirometry, which of the following peak expiratory flow rates will most likely be observed in this patient?
A 9-month-old boy is brought to the physician because of abnormal crawling and inability to sit without support. A 2nd-trimester urinary tract infection that required antibiotic use and a spontaneous preterm birth via vaginal delivery at 36 weeks’ gestation both complicated the mother’s pregnancy. Physical examination shows a scissoring posture of the legs when the child is suspended by the axillae. Examination of the lower extremities shows brisk tendon reflexes, ankle clonus, and upward plantar reflexes bilaterally. When encouraged by his mother, the infant crawls forward by using normal reciprocal movements of his arms, while his legs drag behind. A brain MRI shows scarring and atrophy in the white matter around the ventricles with ventricular enlargement. Which of the following is most likely associated with the findings in this child?
A 5-year-old boy is brought to the physician for excessive weight gain. The mother reports that her son has been “chubby” since he was a toddler and that he has gained 10 kg (22 lbs) over the last year. During this period, he fractured his left arm twice from falling on the playground. He had cryptorchidism requiring orchiopexy at age 2. He is able to follow 1-step instructions and uses 2-word sentences. He is at the 5th percentile for height and 95th percentile for weight. Vital signs are within normal limits. Physical examination shows central obesity. There is mild esotropia and coarse, dry skin. In addition to calorie restriction, which of the following is the most appropriate next step in management of this patient?
A 7-year-old boy is brought to the emergency department by his mother 1 hour after falling off his bike and landing head-first on the pavement. His mother says that he did not lose consciousness but has been agitated and complaining about a headache since the event. He has no history of serious illness and takes no medications. His temperature is 37.1°C (98.7°F), pulse is 115/min, respirations are 20/min, and blood pressure is 100/65 mm Hg. There is a large bruise on the anterior scalp. Examination, including neurologic examination, shows no other abnormalities. A noncontrast CT scan of the head shows a non-depressed linear skull fracture with a 2-mm separation. Which of the following is the most appropriate next step in management?
A 6-year-old boy is brought to the physician because of increasing swelling around his eyes for the past 3 days. During this period, he has had frothy light yellow urine. He had a sore throat 12 days ago. He appears tired. His temperature is 37°C (98.6°F), pulse is 90/min, and blood pressure is 105/65 mm Hg. Examination shows periorbital edema and pitting edema of the lower extremities. Cardiopulmonary examination shows no abnormalities. Which of the following findings on urinalysis is most likely associated with this patient's condition?
A 4-year-old girl is brought to the physician by her parents because she is severely underweight. She is easily fatigued and has difficulty keeping up with other children at her daycare. She has a good appetite and eats 3 full meals a day. She has 4 to 5 bowel movements daily with bulky, foul-smelling stools that float. She has had recurrent episodes of sinusitis since infancy. Her parents report that she recently started to snore during her sleep. She is at the 15th percentile for height and 3rd percentile for weight. Her vital signs are within normal limits. Examination shows pale conjunctivae. A few scattered expiratory crackles are heard in the thorax. There is abdominal distention. Which of the following is the most likely underlying cause of this patient's failure to thrive?
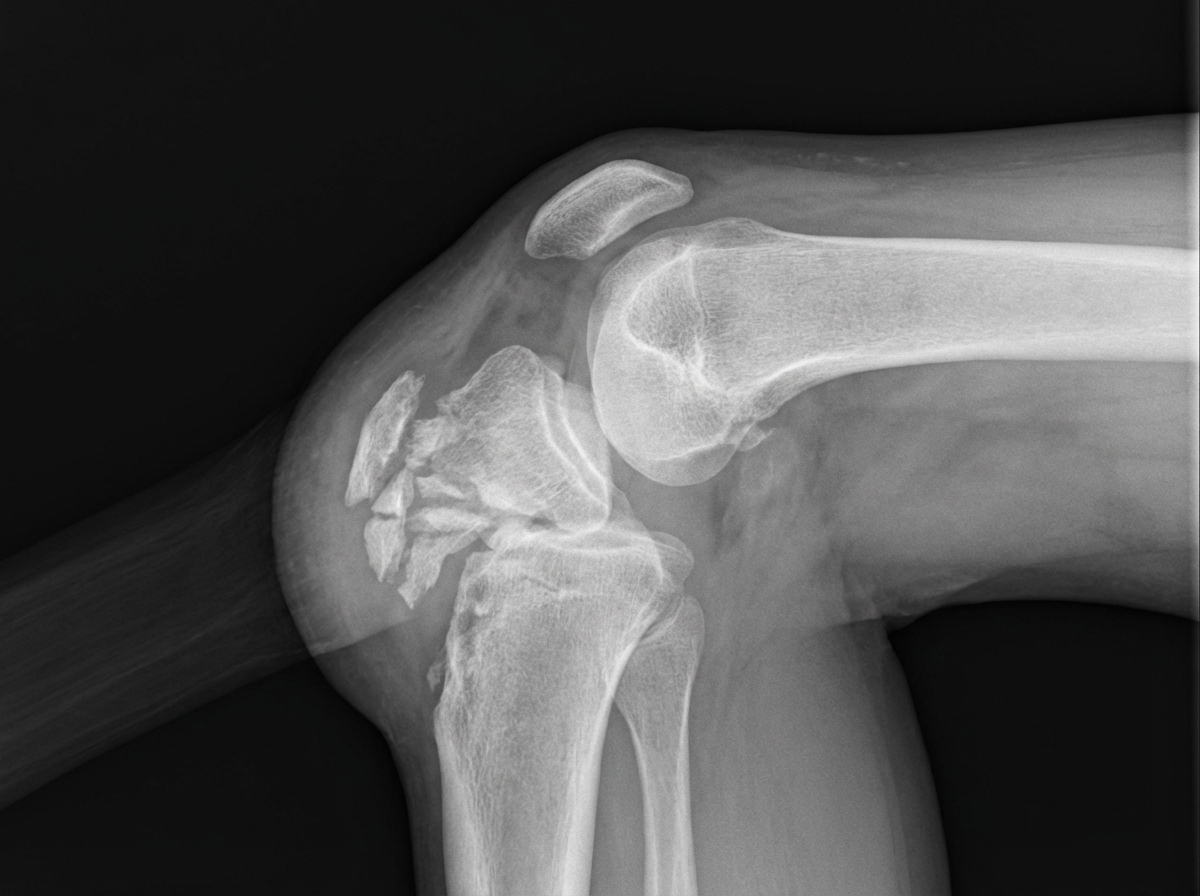
A 12-year-old girl presents to her primary care physician with left knee pain for the past 6 weeks. She recently joined the field hockey team at her school. The pain is the most severe when she is running up and down the stairs at the school stadium. The pain decreases when she goes home and rests after practice. She additionally admits to tripping and landing on her left knee 5 days ago. Physical exam shows a knee with a healing abrasion over the left patella. The tibial tuberosity is tender to palpation. A radiograph of the knee is presented in figure A. Which of the following is the most likely diagnosis?
A 15-month-old girl is brought to the pediatrician by her mother with a history of 3 episodes of breath-holding spells. The patient’s mother says that this is a new behavior and she is concerned. The patient was born at full term by spontaneous vaginal delivery with an uneventful perinatal period. She is also up to date on her vaccines. However, after the age of 6 months, the patient’s mother noticed that she was not as playful as other children of similar age. She is also not interested in interacting with others and her eye contact is poor. Her growth charts suggest that her weight, length, and head circumference were normal at birth, but there have been noticeable decelerations in weight and head circumference. On physical examination, her vital signs are normal. A neurologic examination reveals the presence of generalized mild hypotonia. She also makes repetitive hand wringing motions. Which of the following clinical features is most likely to develop in this patient during the next few years?
A 5-year-old boy presents to the pediatrician for a well child visit. He is meeting his developmental milestones and is in the 15th percentile for height and 70th percentile for weight. His parents report that he complains of fatiguing easily and having trouble participating in sports. They are concerned he is not getting enough sleep and state that sometimes they hear him snore. The patient has a past medical history of a supracondylar fracture of the humerus, which was appropriately treated. He is doing well in school but is sometimes bullied for being small. The patient eats a balanced diet of milk, fruit, and some vegetables. His parents have been trying to get him to drink more milk so he can grow taller. His temperature is 99.5°F (37.5°C), blood pressure is 90/48 mmHg, pulse is 100/min, respirations are 19/min, and oxygen saturation is 98% on room air. On physical exam, the patient appears well. HEENT exam is notable for conjunctival pallor and a unilateral clear middle ear effusion. Cardiac exam reveals a benign flow murmur. Pulmonary exam is clear to auscultation bilaterally. The patient's gait is stable and he is able to jump up and down. A full set of labs are ordered as requested by the parents including a serum vitamin D level, B12 level, and IGF level. A selection of these lab values are seen below. Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 9.9 mg/dL AST: 12 U/L ALT: 10 U/L Which of the following would you expect to find in this patient?
An 8-year-old boy presents with a limp favoring his left leg. The patient's mother noticed he had been limping without complaint for the past 6 months. Past medical history is significant for the flu last year. No current medications. All immunizations are up to date. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 100/60 mm Hg, pulse 74/min, respiratory rate 19/min, and oxygen saturation 99% on room air. The body mass index (BMI) is 17.2 kg/m2. On physical examination, the patient is alert and cooperative. A limp favoring the left leg is noted when the patient is walking. There is mild tenderness on deep palpation of the left lumbar region but no erythema, edema, or warmth. There is a decreased range of motion of the left hip. Which of the following is the most likely diagnosis in this patient?
Practice by Chapter
Normal growth patterns
Practice Questions
Growth charts and interpretation
Practice Questions
Failure to thrive evaluation
Practice Questions
Short stature workup
Practice Questions
Tall stature evaluation
Practice Questions
Obesity in children
Practice Questions
Nutritional assessment tools
Practice Questions
Puberty stages (Tanner stages)
Practice Questions
Precocious puberty
Practice Questions
Delayed puberty
Practice Questions
Growth hormone disorders
Practice Questions
Impact of chronic disease on growth
Practice Questions
Catch-up growth
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app