
Growth/Development — MCQs

On this page
A 26-day-old newborn is brought to the physician because of poor feeding and lethargy for 2 weeks. During this period, he has had a raspy cry. The child was delivered at term at home and has not yet been evaluated by a physician. He is at the 90th percentile for head circumference, 50th percentile for length, and 60th percentile for weight. Vital signs are within normal limits. Examination shows scleral icterus and an enlarged tongue. The abdomen is distended and there is a reducible, soft protruding mass at the umbilicus. Muscle tone is decreased in all extremities. Which of the following is the most likely cause of these findings?
A 2-month-old girl is brought to the physician for a well-child examination. She was born at 32 weeks' gestation and weighed 1616 g (3 lb 9 oz); she currently weighs 2466 g (5 lb 7 oz). She is exclusively breastfed and receives vitamin D supplementation. Physical examination shows no abnormalities apart from low height and weight. This patient is at increased risk for which of the following complications?
A 3-year-old girl is brought to the physician for a well-child examination. She was born at term and has been healthy since. She can climb up and down the stairs and can pedal a tricycle. She has difficulty using a spoon to feed herself but can copy a line. She speaks in 2- to 3-word sentences that can be understood by most people. She is selfish while playing with children her age and throws tantrums quite often. She cannot put on her own shoes and socks. She does not tolerate separation from her parents. She is at 60th percentile for height and weight. Physical examination including neurologic examination reveals no abnormalities. Which of the following is the most appropriate assessment of her development?
A 6-year-old boy presents to the pediatrician with his parents. He is fully vaccinated and met most developmental milestones. His fine motor milestones are delayed; at present, he cannot eat by himself and has difficulty in self-dressing. His intelligence quotient (IQ) is 65. He listens quietly while spoken to and engages in play with his classmates. He neither talks excessively nor remains mute, but engages in normal social conversation. There is no history of seizures and he is not on any long-term medical treatment. On his physical examination, his vital signs are stable. His height and weight are normal for his age and sex, but his occipitofrontal circumference is less than the 3rd percentile for his age and sex. His neurologic examination is also normal. Which of the following is the most likely diagnosis?
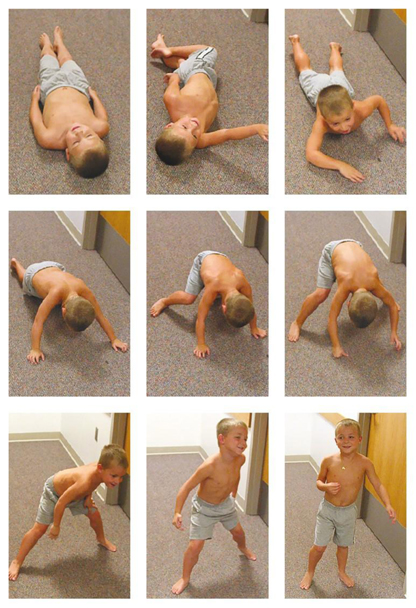
A 4-year-old boy presents with a recent history of frequent falls. The images below depict his movements when he tries to get up from the floor. Which of the following is the most likely diagnosis in this patient?
A 3-year-old boy is brought to the physician because of a 5-day history of yellowing of his eyes and skin. He has had generalized fatigue and mild shortness of breath over the past 2 months. Examination shows pale conjunctivae and scleral jaundice. The spleen is palpated 4 cm below the left costal margin. Laboratory studies show a hemoglobin concentration of 8.5 g/dL and a mean corpuscular volume of 76 μm3. A peripheral blood smear shows round erythrocytes that lack central pallor. Which of the following is the most likely cause of the splenomegaly seen in this child?
A 5-month-old girl is brought to the physician because of a red lesion on her scalp that was first noticed 2 months ago. The lesion has been slowly increasing in size. It is not associated with pain or pruritus. She was born at 37 weeks' gestation after an uncomplicated pregnancy and delivery. Her older sister is currently undergoing treatment for a fungal infection of her feet. Examination shows a solitary, soft lesion on the vertex of the scalp that blanches with pressure. A photograph of the lesion is shown. Which of the following is the most appropriate next step in management?

A 7-year-old girl is brought to the physician by her parents for the evaluation of pubic hair development. She has a history of a fracture in each leg and one fracture in her right arm. Her performance at school is good. There is no family history of serious illness. She takes no medications. Vital signs are within normal limits. Genital examination shows coarse, dark hair along the labia. The breast glands are enlarged and the breast bud extends beyond the areolar diameter. There are several hyperpigmented macules with rough, serpiginous borders of different sizes on the lower and upper extremities. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 13-year-old female comes to your office complaining of dry, scaling skin (Figure A). She is particularly concerned about the appearance of her skin around her peers. She indicates that she did not start having problems until she was 5 years of age, after which her skin has progressively become drier and scalier. She has tried all types of over-the-counter moisturizers with no resolution. What is the most likely diagnosis?

A 2-year-old girl is brought to the physician by her mother for a well-child examination. She is at the 55th percentile for height and the 40th percentile for weight. Vital signs are within normal limits. Physical examination shows no abnormalities. She is able to follow simple commands, such as “close your eyes, then stick out your tongue,” but she is unable to follow 3-step commands. She knows approximately 75 words, and half of her speech is understandable. She can say 2-word phrases, and she is able to name many parts of the body. Assuming normal development, which of the following milestones would be expected in a patient this age?
Practice by Chapter
Normal growth patterns
Practice Questions
Growth charts and interpretation
Practice Questions
Failure to thrive evaluation
Practice Questions
Short stature workup
Practice Questions
Tall stature evaluation
Practice Questions
Obesity in children
Practice Questions
Nutritional assessment tools
Practice Questions
Puberty stages (Tanner stages)
Practice Questions
Precocious puberty
Practice Questions
Delayed puberty
Practice Questions
Growth hormone disorders
Practice Questions
Impact of chronic disease on growth
Practice Questions
Catch-up growth
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app