
Growth/Development — MCQs

On this page
A laborer's younger child is brought to the OPD with a swollen belly and dull face. He has been fed rice water (rice milk) in his diet mostly. On investigations, the child is found to have low serum protein and low albumin. What is the probable diagnosis?
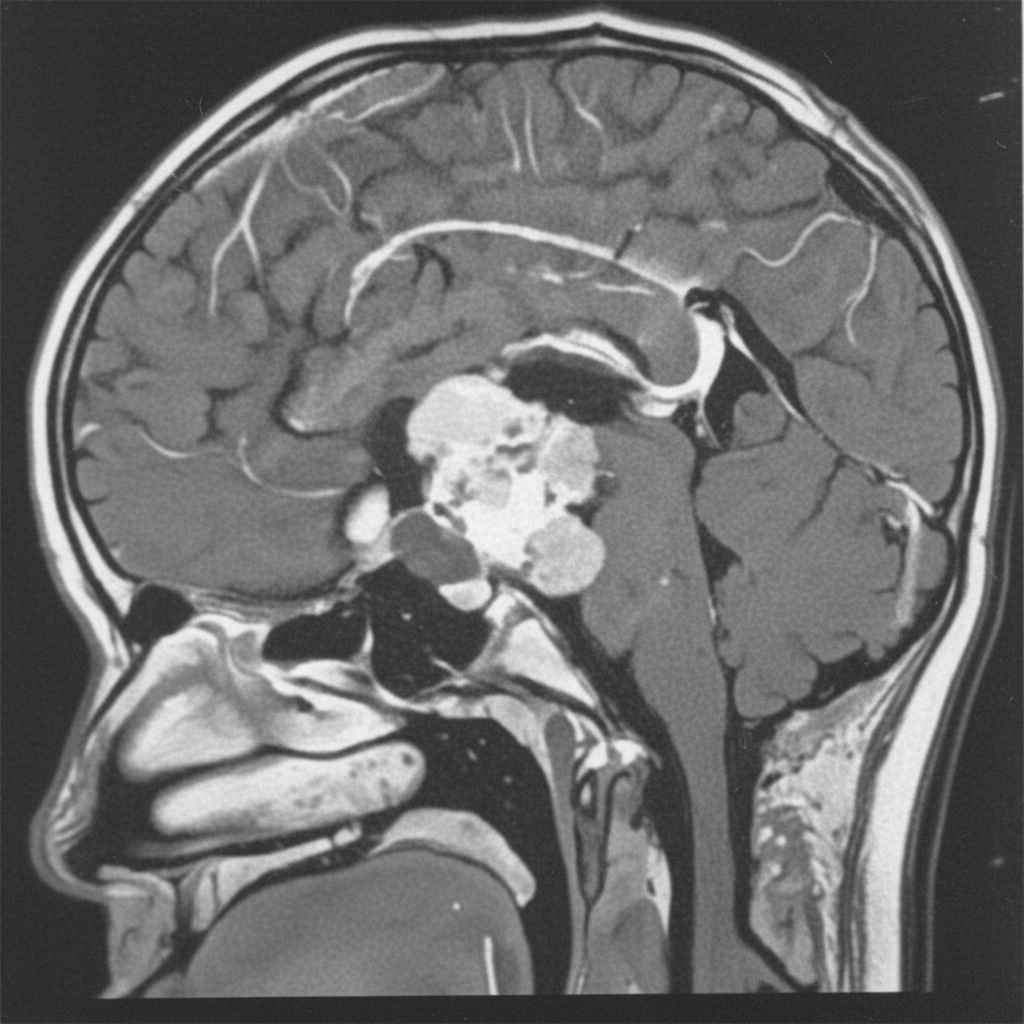
A 12-year-old boy presents with symptoms of headaches, visual disturbances, and growth retardation. An MRI scan is performed, and the image provided shows a cystic mass with both solid and calcified components in the suprasellar region, extending into the third ventricle. Based on the clinical presentation and MRI findings, what is the most likely diagnosis?
A baby was playing unattended and suddenly developed respiratory distress. Based on the X-ray provided, where is the foreign object most likely located?

A 10-year-old child presents with limb pain and recurrent fractures. Bone mineral density is normal, as seen on the X-ray. What is the most likely diagnosis?

An X-ray of a 5-year-old child is shown below. The bone mineral density is normal. What is the most likely diagnosis?

A 10-year-old male presents with generalized edema. His cholesterol level is $238 \mathrm{mg} / \mathrm{dl}$, urine protein is $3+$, and stool microscopy shows fat in the stool. What is the most likely diagnosis?
In a child with a height-for-age Z-score of less than -2 standard deviations (SD), what is the most likely cause?
A child presents with rachitic changes in the limbs that are not responding to Vitamin D supplementation. Investigations reveal the following results: - Calcium: $9.5 \mathrm{mg} / \mathrm{dl}$ - Phosphorus: $1.6 \mathrm{mg} / \mathrm{dl}$ - Alkaline phosphatase (ALP): 814 IU - Serum PTH: $24.2 \mathrm{pg} / \mathrm{ml}$ - Serum electrolytes, creatinine, and blood gases: Normal. What is the most likely diagnosis?
An anganwadi teacher measures the weight and height of a 4-year-old child and finds that the child's height-for-age is below the normal percentile. What does this finding indicate?
A 16-month-old child weighing 8 kg is assessed using a growth chart. The child's weight falls between the median (standard) and minus 2 standard deviations ( -2 SD ). What should be the next step in the management of this child?
Practice by Chapter
Normal growth patterns
Practice Questions
Growth charts and interpretation
Practice Questions
Failure to thrive evaluation
Practice Questions
Short stature workup
Practice Questions
Tall stature evaluation
Practice Questions
Obesity in children
Practice Questions
Nutritional assessment tools
Practice Questions
Puberty stages (Tanner stages)
Practice Questions
Precocious puberty
Practice Questions
Delayed puberty
Practice Questions
Growth hormone disorders
Practice Questions
Impact of chronic disease on growth
Practice Questions
Catch-up growth
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app